Supplements for Thyroid Support
When it comes to the best supplements for thyroid support, the nutrients that work best are typically the ones that a person is deficient in. A thyroid diagnosis is not just a “thyroid gland problem.” Healthy thyroid function depends on a nutrient-dependent hormone system. You need nutritional raw materials to make thyroid hormone, nutritional cofactors to activate it, and adequate gut and liver function to help it do its job. Human studies consistently point to a short list of nutrients that deserve the most attention: selenium, iron, vitamin D, iodine, zinc, B vitamins, protein, and inositol.
A smart thyroid strategy is not to “take everything.” It is to identify where the bottleneck is. Some people struggle with hormone production. Others struggle with conversion of T4 to T3. Others have Hashimoto’s, gut dysfunction, iron depletion, or low vitamin D. That is why the best supplements for thyroid support are the ones that match your actual physiology rather than a generic label.
Also keep in mind that nutrients come from food. And though supplements can be very supportive, a food first approach to getting adequate nutrition should also be your priority.
Contents
ToggleWhy Thyroid Support Should Start With Nutrient Status
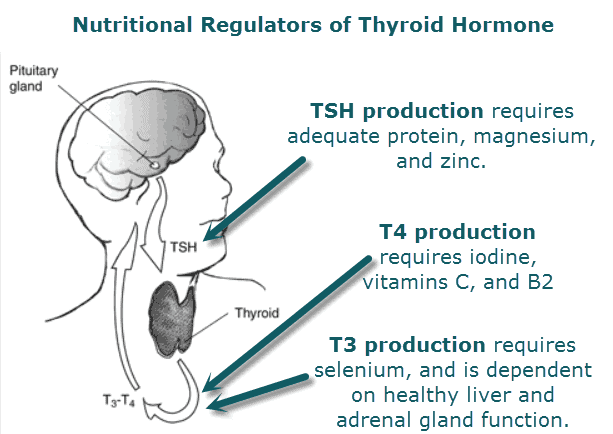
Thyroid hormone production is a stepwise process. The body needs enough iodine and protein to build T4 (inactive thyroid hormone), then it needs selenium and iron to help convert T4 into T3 (active thyroid hormone), and it also relies on nutrients such as magnesium, zinc, vitamin D, vitamin A, vitamin C, and B vitamins to support regulation, signaling, and metabolic response. That broader nutrient cascade is one of the most important practical takeaways in thyroid care.
This matters because many people with low thyroid function or Hashimoto’s are not dealing with a single deficiency. They have a pattern: low ferritin, low vitamin D, marginal selenium, poor protein intake, GI dysfunction, or some combination of those. Reviews of the thyroid literature repeatedly show that micronutrient status influences thyroid hormone synthesis, autoimmune activity, and peripheral hormone metabolism.
In plain English, before you ask, “What are the best supplements for thyroid support?” ask, “What is my thyroid missing?” That approach is better for symptoms, better for precision, and better for long-term results.
The Best Supplements for Thyroid Support
Selenium
If I had to name one of the most researched thyroid support supplements, selenium would be at the top. Selenium is essential for a special enzyme system (deiodinases), that helps convert T4 into the active thyroid hormone, T3. Selenium also acts as a powerful antioxidant defense inside thyroid tissue. That matters because the thyroid is a gland with high oxidative activity.
Human evidence is especially strong in Hashimoto’s. A 2024 systematic review and meta-analysis of randomized controlled trials found that selenium supplementation in Hashimoto’s thyroiditis reduced TSH (thyroid stimulating hormone) in patients not taking thyroid hormone and lowered thyroid peroxidase (TPO) antibodies.
Because it targets both hormone physiology and inflammatory stress, selenium is one of the best supplements for Hashimoto’s and hypothyroidism when low intake, poor status, autoimmunity, or impaired conversion is part of the picture.
How Much Selenium Should You Take? The recommended selenium dosage for nutritionally supporting Hashimoto’s thyroiditis is 100-200 mcg/day. Clinical studies have demonstrated that 200 mcg of selenomethionine daily for periods of 6-12 months reduce anti-thyroid peroxidase (anti-TPO) antibodies and improve well-being.
Iron
Iron is often underappreciated in thyroid care, especially for women with heavy menstrual losses, endurance athletes, postpartum women, and anyone with chronic gut issues. Iron is essential because the enzyme (TPO – thyroid peroxidase is iron-dependent) that helps activate your thyroid hormone.
A 2023 review concluded that published studies show a direct relationship between iron deficiency, thyroid function, and thyroid autoimmunity. A 2021 systematic review and meta-analysis also identified iron deficiency as a risk factor for thyroid disorders in women. Iron deficiency was linked to elevated antibodies, TSH, and low T4 levels.
This is why iron deficiency and thyroid function belong in the same conversation. If iron and ferritin are low, thyroid function may suffer.
How Much Iron Should You Take? Before taking higher doses of iron, always consider testing first. Too much iron can become damaging instead of beneficial. Ask your doctor to run an iron panel with ferritin first. If your iron levels are low, consider starting with 60-120 mg/day.
A couple of other factors to consider with iron:
- Iron deficiency is the #1 reported nutritional deficiency for those with gluten sensitivity and celiac disease.
- If you are menstruating, struggle with chronic inflammation, or have occult blood in your stool or urine, you are at greater risk for iron deficiency.
- Iron is better absorbed with vitamin C, and works better when copper is adequate. The take away here is – find an iron supplement with vitamin C and copper in it as well to take advantage of the synergism between these nutrients.
Vitamin D
Vitamin D is more than a bone nutrient. It is an immune-regulating hormone-like nutrient, and that makes it highly relevant in Hashimoto’s thyroiditis. Low vitamin D status is common in autoimmune thyroid disease, and supplementation has shown benefit in several controlled human research studies.
It is important to not that these studies showed that supplementation of vitamin D was only effective if vitamin D3 (cholecalciferol) was used. Additionally, supplementation was necessary for at least three months.
How Much Vitamin D Should You Take? Doses ranging between 4,000 – 10,000 IU/day have been used safely. If you are taking higher doses, make sure to ask you doctor for a 25 OHD blood test to monitor your levels. Look for an emulsified (mixed in oil) form of cholecalciferol as it is better absorbed.
Inositol
Inositol is a nutrient required for hormone signaling. In relation to the thyroid, myo-inositol helps TSH to effectively stimulate the production of thyroid hormone.
A 2013 study found that myo-inositol plus selenium improved thyroid function in subclinical hypothyroidism, and a 2017 study reported restoration toward euthyroidism in Hashimoto’s patients with subclinical hypothyroidism after combination treatment. A 2025 review also concluded that the combination may reduce antibodies and improve thyroid function more effectively than selenium alone.
How Much Inositol Should I Take? Research studies have used 600 mg/day myo-inositol specifically for up to 6 months. Supplementation is very safe. As with any supplement program, talk with your doctor if you aren’t sure if it is right for you.
Iodine
Iodine should not be feared. It should be respected. The thyroid cannot make thyroid hormone without it. T4 literally contains four iodine atoms, and T3 contains three. That makes iodine foundational, not optional.
At the same time, iodine works best in context. Reviews on thyroid nutrition consistently note that iodine interacts with selenium, iron, and vitamin A. In other words, iodine is often part of a network, not a solo act.
Many argue that iodine can be problematic for people with autoimmune thyroid disease (AITD). Others argue that iodine supplementation has nothing to do with increased AITD. In my experience the latter is true. Iodine supplementation is often necessary. The key take away is: Test, Don’t Guess. Iodine levels can be measure accurately through both iodine loading tests as well as INA testing.
How Much Iodine Should I Take? Typical higher dose iodine recommendations range from 12-25 mg/day. Look for an iodine supplement that contains both molecular iodine and potassium iodide. It is always a good idea to take iodine under the supervision of a nutritional expert.
Zinc and Copper
Zinc is one of the better-supported trace minerals for thyroid support. It contributes to thyroid hormone metabolism and appears to positively influence T3 levels in some human studies. A 1999 study found that zinc sulfate supplementation improved thyroid function in zinc-deficient children with Down syndrome and subclinical hypothyroidism. Human studies also show that zinc supplementation improves free T-3 in overweight and obese people.
Copper gets less attention, but it plays an important role in thyroid hormone metabolism. Zinc and copper work together to drive the antioxidant systems (SOD) in the body that are protective to the thyroid.
How much Zinc Should I Take? Typical zinc dosing ranges from 25-100 mg/day. Copper dosing can range from 2-4 mg/day. It is best to measure both nutrients before supplementing with higher doses for long periods of time.
B Vitamins
B vitamins deserve more respect in thyroid care. They help support energy production, nervous system function, methylation, and in some cases may affect how your doctor interprets your thyroid blood tests.
B vitamins are especially important if you are taking thyroid hormone replacement therapy (such as levothyroxine). These medications can accelerate metabolic processes that consume B vitamins, potentially leading to or worsening deficiencies, particularly when metabolic rates increase faster than nutrient intake. Because B vitamins act as co-enzymes in energy metabolism, the increased cellular demand for energy can rapidly deplete stored B vitamins.
Vitamin B12: A 2023 systematic review and meta-analysis found that patients with hypothyroidism had lower vitamin B12 levels than healthy controls. Separate studies and reviews also report a meaningful prevalence of B12 deficiency in autoimmune thyroid disease, likely due in part to overlap with autoimmune gastritis or pernicious anemia in some patients.
Folate: A 2025 study showed higher incidence of autoimmune thyroid disease (AIT) in people who consumed less folate. The authors of the study conclude ” that lower dietary folate intake may be an independent factor contributing to AIT.” Another study found lower levels of folate in hypothyroid patients. The authors of the study recommended that patients with hypothyroid have their folate status checked and monitored.
Vitamin B6:
This is why vitamins for thyroid support should not be reduced to one bottle labeled “thyroid.” B12, and often B2 and B3 from a mechanistic standpoint, belong in the conversation.
Protein
The thyroid does not run on trace minerals alone. It also needs amino acids. Phenylalanine and tyrosine can be found in many protein sources and are used to make thyroxine (T4), making it essential for thyroid hormone production. Thyroglobulin and thyroid hormone formation depend on amino acid structure, and adequate protein intake supports the raw-material side of hormone production.
This matters more than many people realize. Patients who under eat, follow a low protein, adhere to plant based diets, or rely heavily on ultra-processed foods can easily end up with enough calories to survive but not enough amino acid nutrition to thrive. For people searching what nutrients are needed for thyroid hormone production, protein belongs on the list.
Vitamin C
Vitamin C is rarely the headline nutrient in thyroid articles, but it has useful support in the literature. One important clinical trial showed that in hypothyroid patients with gastrointestinal pathology, vitamin C improved levothyroxine absorption enough to improve TSH, free T4, and T3 measurements.
That makes vitamin C interesting for two reasons. First, it may support the chemistry and transport environment around thyroid hormone production. Second, it may help some patients absorb medication more effectively when low stomach acid or GI dysfunction is part of the story.
Magnesium, Vitamin A, and Omega-3s
These are not always the first nutrients discussed, but they are essential in thyroid hormone production. Reviews of thyroid nutrition consistently include magnesium and vitamin A among nutrients influencing thyroid physiology, and randomized work suggests that zinc, vitamin A, and magnesium may produce beneficial effects in hypothyroid states.
Omega-3s also deserve attention. The thyroid is an inflammatory target in autoimmune disease, and omega-3 status may influence immune tone, membrane signaling, and metabolic response. The human thyroid literature on omega-3s is not as deep as the selenium literature, but reviews continue to identify omega-3 fats as supportive nutrients in thyroid-related metabolic health.
If you are looking for natural thyroid support supplements, this trio is best viewed as foundational support rather than a one-step fix.
Probiotics and the Gut-Thyroid Axis
The thyroid and the gut talk to each other. Gut bacteria influence immune signaling, nutrient absorption, intestinal permeability, and the enterohepatic handling of thyroid-related compounds. That is why the gut-thyroid axis has become a major theme in thyroid research.
Human intervention data on probiotics are mixed, but still clinically interesting. A 2017 trial found that probiotics did not directly change thyroid compensation in a major way, yet they appeared to stabilize thyroid hormone fluctuations. A 2024 meta-analysis found that probiotics and prebiotics positively influence antibody activity in Graves’ disease.
So where do probiotics fit? They are not a replacement for selenium, iron, vitamin D, or iodine. But for people with Hashimoto’s plus bloating, IBS, constipation, antibiotic history, or obvious gut dysfunction, they can be a very reasonable part of a thyroid support supplements strategy.
Dr. Osborne’s Top Nutritional Supplements For Thyroid Support
| Nutrient | Why It Matters for Thyroid Support | Practical Dose Range |
|---|---|---|
| Selenium | Supports conversion of T4 into active T3 and helps protect thyroid tissue from oxidative stress. | 100–200 mcg/day |
| Iron | Needed for thyroid hormone production and conversion. Low iron can impair thyroid performance and is especially relevant when ferritin is low. | 60–120 mg/day when iron is low |
| Vitamin D3 | Helps support immune balance and is especially relevant in autoimmune thyroid patterns such as Hashimoto’s. | 4,000–10,000 IU/day |
| Myo-Inositol | Supports thyroid signaling and has been studied in combination with selenium for subclinical hypothyroid and autoimmune thyroid patterns. | 900-1800 mg/day |
| Iodine | A core raw material used to build thyroid hormone. Adequate iodine is necessary for normal thyroid hormone production. | 150 mcg/day for basic support; 12–25 mg/day in higher-dose thyroid protocols |
| Zinc | Plays a role in thyroid signaling, hormone regulation, and immune support. | 25–100 mg/day |
| Copper | Helps support antioxidant systems and mineral balance relevant to thyroid physiology. | 2–4 mg/day |
| Vitamin B12 | Supports neurologic function, energy metabolism, and upstream thyroid signaling. | 1,000–5,000 mcg/day |
| Vitamin B2 | Helps support energy metabolism and participates in pathways involved in thyroid hormone production. | 10–50 mg/day |
| Vitamin B3 | Supports cellular energy production and helps with pathways tied to iodine utilization and thyroid hormone synthesis. | 50–250 mg/day |
| Protein / Tyrosine | Protein provides amino acids needed to build thyroid hormone. Tyrosine is one of the main raw materials used in thyroid hormone formation. | Protein: 0.8 – 1 gram/lbs lean body weight; L-tyrosine: 1,500–2,000 mg/day |
| Vitamin C | Supports thyroid hormone production pathways and may also help support iron utilization. | 500–2,000 mg/day |
| Magnesium | Supports thyroid signaling and broader energy metabolism. | 200–600 mg/day |
| Vitamin A | Helps active thyroid hormone communicate with cells and support metabolic response. | 2,500–10,000 IU/day |
| Omega-3s | Support inflammatory balance, cell membrane health, and the body’s metabolic response to thyroid hormone. | 1–3 g/day combined EPA + DHA |
| Probiotics | Support the gut-thyroid axis by helping regulate gut flora, digestion, and nutrient handling. | 100–200+ billion CFU/day |
**This chart is designed for educational purposes only. It is not intended to be used as medical advice or a replacement for your medication. Always speak with your doctor before starting a nutritional supplement program. Testing for nutritional deficiencies Vs. blind supplementation is recommended.
Supplements That Can Cause False Alarm When Getting Your Thyroid Tests Performed
Iodine and biotin supplementation before having your blood drawn may interfere with the accuracy of your lab tests. High-dose biotin (often in hair/skin supplements) commonly causes falsely elevated T3/T4, and falsely low TSH levels, mimicking hyperthyroidism. High dose iodine supplementation can cause false elevations in your TSH mimicking hypothyroid disease.
The best practice with iodine and biotin supplementation is to avoid using high doses of either 3-7 days prior having your labs drawn.
Thyroid Medication Interactions With Supplements
This is one of the most important parts of the whole discussion. Some of the very nutrients that support thyroid health can interfere with levothyroxine if taken too close together.
The American Thyroid Association (ATA) notes that iron, calcium, soy, certain antacids, and some other drugs or supplements can reduce absorption of thyroid hormone. ATA patient education materials also explain that levothyroxine absorption is decreased when taken with calcium, iron, and some foods or medications. The NIH Office of Dietary Supplements likewise notes that taking iron with levothyroxine can reduce the medication’s effectiveness, and chromium can also reduce levothyroxine absorption when taken at the same time.
That means supplements can still be used. You just separate them. For many patients, the cleanest strategy is to take thyroid medication by itself on an empty stomach, then take minerals later in the day. That preserves medication absorption while still allowing you to build a meaningful nutrient protocol.
Vitamin C is a notable exception worth remembering because one trial showed it may improve levothyroxine absorption in patients with GI pathology.
How to Test Before You Supplement
If you want a the most effective supplements for low thyroid function, test, don’t guess.
For thyroid hormones, that means a full panel rather than TSH alone. For thyroid autoimmunity, that means checking thyroid peroxidase antibodies and thyroglobulin antibodies when Hashimoto’s is in the conversation. For nutrient status, the highest-yield targets are usually vitamin D, iron studies with ferritin, B12, zinc, and in the right patient, iodine and selenium status. The overall thyroid literature strongly supports the importance of iodine, iron, selenium, zinc, copper, vitamin D, vitamin A, and B12 in thyroid physiology.
This matters for women in particular. Thyroid support for women often intersects with menstrual iron loss, postpartum depletion, autoimmune disease, dieting history, gut dysfunction, and vitamin D insufficiency. In many cases, what looks like a thyroid problem is partly a nutrient problem.
The more precise testing you have done, the more precise your support plan becomes. That is how you stop guessing and start building a thyroid strategy that actually makes sense.
Best Lab Tests for Thyroid Support
| Test | Type of Test | What It Measures | Why It Matters | Ideal Use Case |
|---|---|---|---|---|
| TSH | Standard thyroid marker | Pituitary signaling to the thyroid gland | Useful as a starting point, but it is only a signaling hormone and not actual thyroid hormone. It should not be used alone to make the whole decision. | First-pass screening for possible hypo- or hyperthyroid patterns |
| Total T4 | Standard thyroid marker | Total thyroxine in circulation, including bound and unbound hormone | Helps show how much thyroid hormone is being produced overall. | Baseline assessment of thyroid output |
| Total T3 | Standard thyroid marker | Total triiodothyronine in circulation, including bound and unbound hormone | Gives a broader look at actual levels of the active thyroid hormone . | Helpful when energy, metabolism, and symptoms do not match TSH alone |
| Free T4 | Standard thyroid marker | Unbound T4 available for conversion and tissue use | Helps assess how much thyroid hormone is available to be converted into active T3. | Suspected production issues or incomplete thyroid panel workups |
| Free T3 | Standard thyroid marker | Unbound active thyroid hormone | One of the most practical markers for understanding how much active thyroid hormone is available at the tissue level. | Fatigue, constipation, hair loss, low body temperature, stubborn hypothyroid symptoms |
| Reverse T3 | Standard thyroid marker | Inactive form of T3 | Helps reveal whether T4 is being shunted away from active T3 production and into an inactive form. The transcript also emphasizes its value when routine labs do not explain symptoms. | Suspected poor T4-to-T3 conversion, lingering symptoms despite “normal” routine labs |
| TPO antibodies | Autoimmune thyroid marker | Antibodies against thyroid peroxidase | Helps identify autoimmune thyroid activity, especially Hashimoto’s thyroiditis. | Family history or suspicion of autoimmunity, fluctuating thyroid labs, suspected Hashimoto’s |
| Anti-thyroglobulin antibodies | Autoimmune thyroid marker | Antibodies against thyroglobulin | Adds depth to autoimmune screening and can detect thyroid immune activity that a basic hormone panel misses. | Suspected Hashimoto’s even when TPO antibodies are negative or borderline |
| Iron panel | Standard nutrient marker | Usually includes serum iron, TIBC, transferrin saturation, and related indices | Iron is necessary for thyroid hormone production and conversion. Low iron can be a major reason thyroid support is not working. | Fatigue, hair loss, heavy menstrual cycles, restless legs, poor thyroid response |
| Ferritin | Standard nutrient marker | Iron storage | Ferritin helps reveal whether you have enough stored iron to support normal thyroid physiology. | Women with menstrual losses, postpartum depletion, chronic fatigue, low thyroid symptoms |
| 25-OH Vitamin D | Standard nutrient marker | Main storage form of vitamin D | Vitamin D is highly relevant in autoimmune thyroid patterns and immune balance. | Hashimoto’s, immune dysfunction, low sunlight exposure, chronic inflammation |
| INA (Intracellular Nutrient Analysis) | Specialized nutrient test | Functional intracellular assessment of more than 50 nutrients | Goes deeper than routine serum testing by looking at what is actually happening inside the cell. Particularly valuable for assessing all B vitamins, selenium, zinc, copper, vitamin A, magnesium, and inositol, along with many other nutrients tied to thyroid hormone production, conversion, and signaling. | People with persistent symptoms, complex cases, Hashimoto’s, suspected multiple deficiencies, poor response to medications and generic thyroid supplements. |
| Halide Loading Test | 24 hour urine collection after a 50 mg iodine dose. | Iodine status as well as fluoride and bromine | Helpful to discern tissue storage of iodine. Also helps to understand whether fluoride or bromine excess may be contributing to iodine deficiency | Poor iodine diet, high fluoride and bromine exposure through toothpaste, water, or pesticides. |
How to use this chart
A complete thyroid nutrition strategy should answer four questions:
- Is the brain signaling the thyroid properly?
Look at TSH. - Is the thyroid producing enough hormone?
Look at Total T4, Free T4, Total T3, Free T3 and reverse T3. - Is there autoimmune thyroid damage?
Look at TPO antibodies and anti-thyroglobulin antibodies. - Is nutrient depletion blocking the system?
Look at iron panel, ferritin, 25-OH vitamin D, and INA.
The best way to choose supplements for thyroid support is to test the entire thyroid pathway, including hormone production, hormone conversion, thyroid antibodies, iron status, vitamin D, and intracellular nutrient reserves.
FAQ: Supplements for Thyroid Support
What are the best supplements for thyroid support?
The best-supported options in the human literature are selenium, iron when deficient, vitamin D, iodine when intake or status is low, zinc, and the combination of inositol plus selenium in selected Hashimoto’s or subclinical hypothyroid cases. Probiotics, B12, magnesium, vitamin A, omega-3s, vitamin C, and adequate protein can also be valuable depending on the person.
Which vitamins help thyroid function naturally?
Vitamin D, B vitamins, vitamin A, vitamin C, and inositol are all essential nutrients for healthy thyroid hormone stimulation, production, and function..
What nutrients are needed for thyroid hormone production?
Iodine and protein are the key raw materials, while selenium and iron are critical for hormone conversion. Omega 3 fatty acids, zinc, copper, magnesium, vitamin D, vitamin A, vitamin C, and B vitamins also influence thyroid function and signaling.
What are the best supplements for Hashimoto’s and hypothyroidism?
For Hashimoto’s, selenium, vitamin D, iron when deficient, and myo-inositol plus selenium have the strongest support. For hypothyroidism more broadly, the best nutrient choices depend on whether the main issue is production, conversion, autoimmunity, or medication absorption. The best supplements are the one’s that the patient needs.
Can iodine make hypothyroidism worse?
Too much iodine can create problems in susceptible people, but iodine is still essential for making thyroid hormone. The right takeaway is not to fear iodine. It is to use iodine with context, preferably after appropriate testing and a broader nutrient assessment that includes selenium and iron.
What supplements interfere with levothyroxine?
Iron, calcium, soy, certain antacids, chromium, and some other products can reduce levothyroxine absorption if taken too close together. Usually the answer is not to avoid them altogether, but to separate timing.
Are probiotics good for thyroid support?
They can be, especially when gut dysfunction is part of the picture. The strongest reason to use them is not that they reliably raise thyroid hormone levels, but that they may help gut ecology, nutrient handling, and immune balance along the gut-thyroid axis.
Do I need to test before taking thyroid support supplements?
That is the best way to do it. Testing helps you identify whether you need iron, vitamin D, selenium, B12, iodine, zinc, or a different strategy entirely. Precision beats guesswork.
Can gluten cause hypothyroidism?
Another major contributor to hypothyroidism is gluten. It is known to directly contribute to Hashimoto’s and low thyroid, but it can also indirectly affect the thyroid by causing malnutrition. This occurs because gluten sensitivity can damage the intestinal lining and block the absorption of key nutrients for this organ. The top two deficiencies include iron and B12 which are both necessary for this organ to function properly.
Can coffee cause thyroid problems?
Coffee can reduce the impact and effectiveness of thyroid medications. Furthermore, the proteins in coffee can mimic gluten, which is a known contributor to this disease.