new to the gluten free journey?

Peripheral neuropathy (PN) is a common reason people seek medical care, but the diagnostic workup is often incomplete. A 2025 JAMA Neurology study found that key tests for treatable causes are underused. As a result, many patients may be labeled with “idiopathic” peripheral neuropathy and placed on symptom suppressing medication while the real root cause goes unidentified and untreated. It is estimated the 25-46% of all cases of peripheral neuropathy fall in the category of idiopathic (unknown cause).
Because of this, PN is often treated like a pain problem. A patient suffers with burning feet, electric shocks, pins and needles, numbness, or balance changes. They go to the doctor. They may be told their MRI’s and labs are “normal.” The prescription pad comes out, the patient is put on life long medication, and the investigation ends. And because this scenario is so common, you need to make sure you are educated and prepared when you visit your doctor.

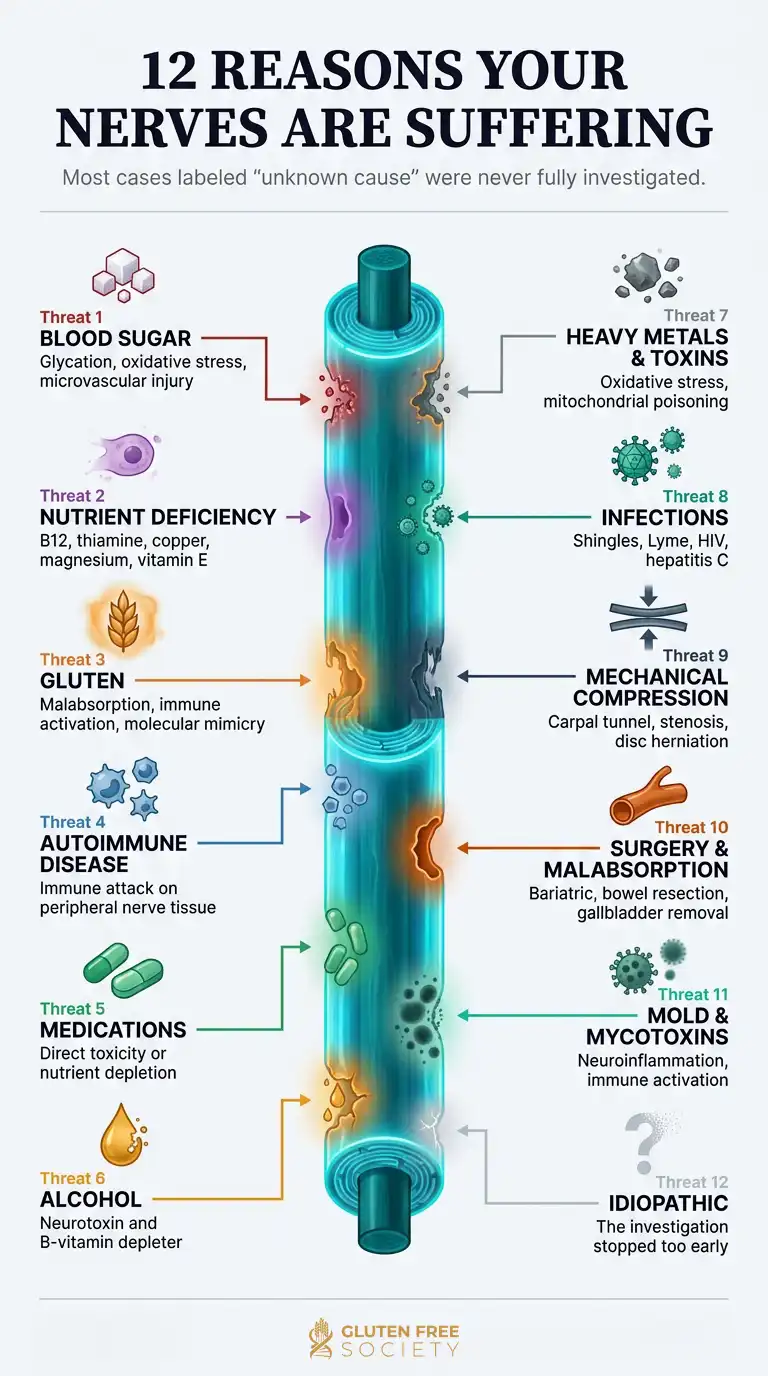
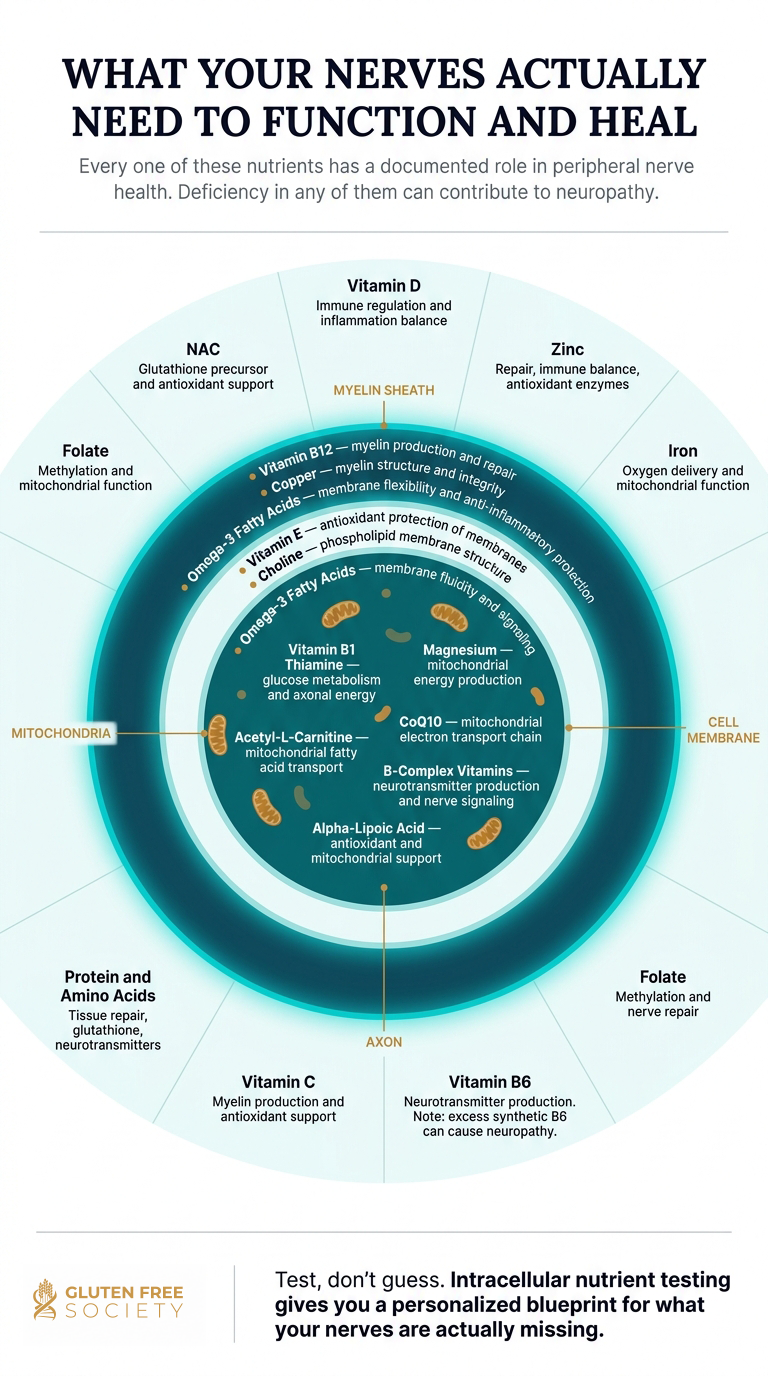
Simply put, peripheral neuropathy means the nerves outside the brain and spinal cord have been damaged. To function properly, peripheral nerves need oxygen, blood flow, mitochondrial energy, healthy fats, amino acids, antioxidants, minerals, and B vitamins. They can be injured by high blood sugar, autoimmune inflammation, gluten-related immune activation, nutrient deficiencies, medications, alcohol, chemotherapy, infections, toxins, mold-related inflammatory burden, physical trauma, and mechanical compression.
| Category | Key Details |
|---|---|
| Condition name | Peripheral neuropathy – additional terms include polyneuropathy, nerve damage, neuritis, idiopathic neuropathy |
| Basic definition | Damage or dysfunction of peripheral nerves outside the brain and spinal cord |
| Common symptoms | Burning, numbness, tingling, stabbing pain, electric shocks, weakness, balance problems, hypersensitivity |
| Common nerve types affected | Sensory, motor, autonomic |
| Common root causes | Diabetes, prediabetes, nutrient deficiency, gluten sensitivity, celiac disease, autoimmunity, medications, alcohol, toxins, infections, compression |
| Nutrient deficiencies linked to neuropathy | B12, B1, B6, folate, vitamin E, vitamin C, copper, magnesium, vitamin D, iron, omega-3 fats, amino acids |
| Gluten-related mechanisms | Malabsorption, immune activation, inflammation, antibody-mediated neurological injury, gut barrier dysfunction |
| Autoimmune mechanisms | Immune attack against nerves, inflammatory neuropathy, small fiber neuropathy, systemic inflammation |
| Blood sugar mechanisms | Glycation, oxidative stress, microvascular damage, mitochondrial dysfunction, inflammation |
| Medication-related causes | Metformin, PPIs, chemotherapy, fluoroquinolones, nitrofurantoin, anticonvulsants, diuretics, steroids, alcohol |
| Toxin-related causes | Heavy metals, mycotoxins, solvents, pesticides, chemotherapy, alcohol, environmental toxins |
| Helpful Diagnostic tests | Neurological exam, EMG/NCS, skin biopsy, A1c, fasting insulin, glucose tolerance, B12, MMA, homocysteine, B1, B6, copper, vitamin D, vitamin E, omega-3 index, intracellular nutrient testing (INA), gluten testing, autoimmune markers |
| Useful food strategies | Grain-free, high-protein, nutrient-dense, low-sugar, anti-inflammatory, rich in animal protein, seafood, organ meats, vegetables, healthy fats, fruit |
| Targeted supplement categories | B12, B-complex, benfotiamine, magnesium, omega-3, vitamin D, vitamin E, vitamin C, copper, zinc, alpha-lipoic acid, acetyl-L-carnitine, NAC, amino acids |
| Red flags needing urgent evaluation | Rapid weakness, paralysis, loss of bowel or bladder control, severe back pain with neurological deficits, stroke-like symptoms, inability to walk, rapidly spreading numbness |
| Commonly Misdiagnosed | Leads to mistreatment and persistent progression of the problem. Root cause investigation should be the top priority for patients and their doctors. |
Peripheral neuropathy is a broad term for damage or dysfunction in the peripheral nervous system. The central nervous system includes the brain and spinal cord. The peripheral nervous system includes the nerves that branch out from the spine and travel into the arms, hands, legs, feet, skin, muscles, organs, blood vessels, and digestive tract.
These nerves help you:
When peripheral nerves are irritated, inflamed, undernourished, compressed, poisoned, or attacked by the immune system, symptoms can show up in many ways.
A person might feel burning feet at night. Another might notice numb toes. Someone else may have tingling hands, stabbing pain, electric shocks, weak grip, foot drop, digestive motility problems, abnormal sweating, dizziness when standing, or poor balance.
Peripheral neuropathy tells you the nerves are irritated, injured, inflamed, compressed, undernourished, poisoned, or being attacked. The label is not the end of the investigation. It is the beginning.
Peripheral nerves do different jobs.
Sensory nerves carry information about touch, pain, vibration, temperature, and body position. Damage here can cause numbness, tingling, burning, stabbing pain, hypersensitivity, or loss of protective sensation.
Motor nerves control muscles. Damage here can cause weakness, cramps, twitching, foot drop, muscle wasting, poor coordination, and difficulty walking.
Autonomic nerves control automatic body functions. Damage here can affect digestion, sweating, bladder function, sexual function, heart rate, and blood pressure.
Many people have mixed neuropathy, where more than one nerve type is affected.
Large fiber nerves help with vibration sense, balance, reflexes, and position awareness. These problems are often detected on neurological exam, EMG, MRI imaging, or nerve conduction testing.
Small fiber nerves carry pain, temperature, and autonomic signals. Small fiber neuropathy can cause burning, prickling, temperature sensitivity, and autonomic symptoms. Standard nerve conduction studies can be normal because they mainly evaluate large nerve fibers. Skin biopsy and specialized autonomic testing can help confirm small fiber neuropathy.
Key Takeaway: A normal EMG or MRI does not always mean the nerves are healthy. Small fiber neuropathy can be missed when testing is incomplete.
Sensory neuropathy is the form most people recognize first. It often begins in the feet or toes and can move upward over time.
Common symptoms include:
Loss of protective sensation is dangerous. If you cannot feel the bottom of your feet well, you may not notice cuts, burns, blisters, ulcers, or injuries.
Motor neuropathy affects muscle control.
Symptoms may include:
Motor symptoms deserve careful evaluation, especially when they are progressive.
Autonomic neuropathy, sometimes referred to as dysautonomia affects automatic functions.
Symptoms can include:
Autonomic involvement can occur in diabetes, autoimmune disease, small fiber neuropathy, infections, and other inflammatory states.
Small fiber neuropathy often causes burning pain, prickling, temperature sensitivity, and autonomic symptoms. It may occur with diabetes, prediabetes, autoimmune disease, celiac disease, gluten sensitivity, infections, medications, or toxin exposure.
Nerve conduction studies often miss small fiber neuropathy. The frustrating part is that a person can have severe burning pain and still have a “normal” nerve conduction study.
Large fiber neuropathy may cause:
Large fiber neuropathy is often easier to detect with standard neurological testing.
Mononeuropathy affects one nerve. Examples include carpal tunnel syndrome, ulnar neuropathy, peroneal nerve palsy, or tarsal tunnel syndrome.
Polyneuropathy affects many nerves, often in a stocking-glove pattern beginning in the feet and later affecting the hands.
Chronic neuropathy may develop slowly over months or years.
Acute or rapidly progressive neuropathy requires more urgent evaluation, especially when weakness, paralysis, breathing difficulty, loss of walking ability, bowel or bladder dysfunction, or stroke-like symptoms are present.
| Body System / Nerve Function | Possible Neuropathy Symptoms |
|---|---|
| Feet and toes | Burning, numbness, tingling, cold sensations, stabbing pain, loss of feeling |
| Hands and fingers | Pins and needles, weak grip, numb fingertips, dropping objects |
| Pain perception | Electric shocks, stabbing pain, shooting pain, hypersensitivity |
| Balance and coordination | Wobbling, falls, trouble walking in the dark, poor position sense |
| Muscles | Weakness, cramps, twitching, foot drop, muscle wasting |
| Reflexes | Reduced ankle reflexes, slower response |
| Skin and temperature | Hot or cold sensations, inability to sense heat, color changes |
| Digestion | Constipation, diarrhea, bloating, gastroparesis |
| Bladder | Urgency, retention, incomplete emptying |
| Heart rate / blood pressure | Dizziness when standing, rapid heart rate, blood pressure swings |
| Sexual function | Erectile dysfunction, reduced sensation |
| Sleep | Burning feet at night, pain waking the person from sleep |
| Mood and cognition | Anxiety, irritability, poor sleep, brain fog from chronic pain or inflammation |
Early onset neuropathy may feel mild:
Early symptoms are often dismissed as aging, poor circulation, anxiety, or “just diabetes.” That is a mistake. Early warning signs are the best opportunity to investigate the cause.
Advanced neuropathy symptoms may include:
Seek urgent evaluation when neuropathy symptoms include:
Peripheral neuropathy is not one disease. It is a pattern of nerve dysfunction that can come from many root causes. The National Institute for Neurological Disorders and Stroke lists diabetes, autoimmune disease, infections, inherited disorders, tumors, bone marrow disorders, kidney disease, liver disease, hypothyroidism, toxins, nutritional deficiencies, alcohol use, medications, and physical injury among potential contributors.
In reality, neuropathy is often multifactorial. One person may be gluten sensitive, have prediabetes, take metformin, have low B12, and eat a processed food diet. Another may have autoimmune disease, thyroid dysfunction, low protein intake, mold exposure, and medication-induced nutrient depletion.
Because of its multifactorial nature, it is important to understand all of your triggers, and have a meaningful discussion with your doctor. This allows for greater discernment, and a more meaningful treatment plan. A plan based on your unique triggers. A plan that addresses the root cause(s).
| Root Cause Category | How It Can Damage Nerves | Examples |
|---|---|---|
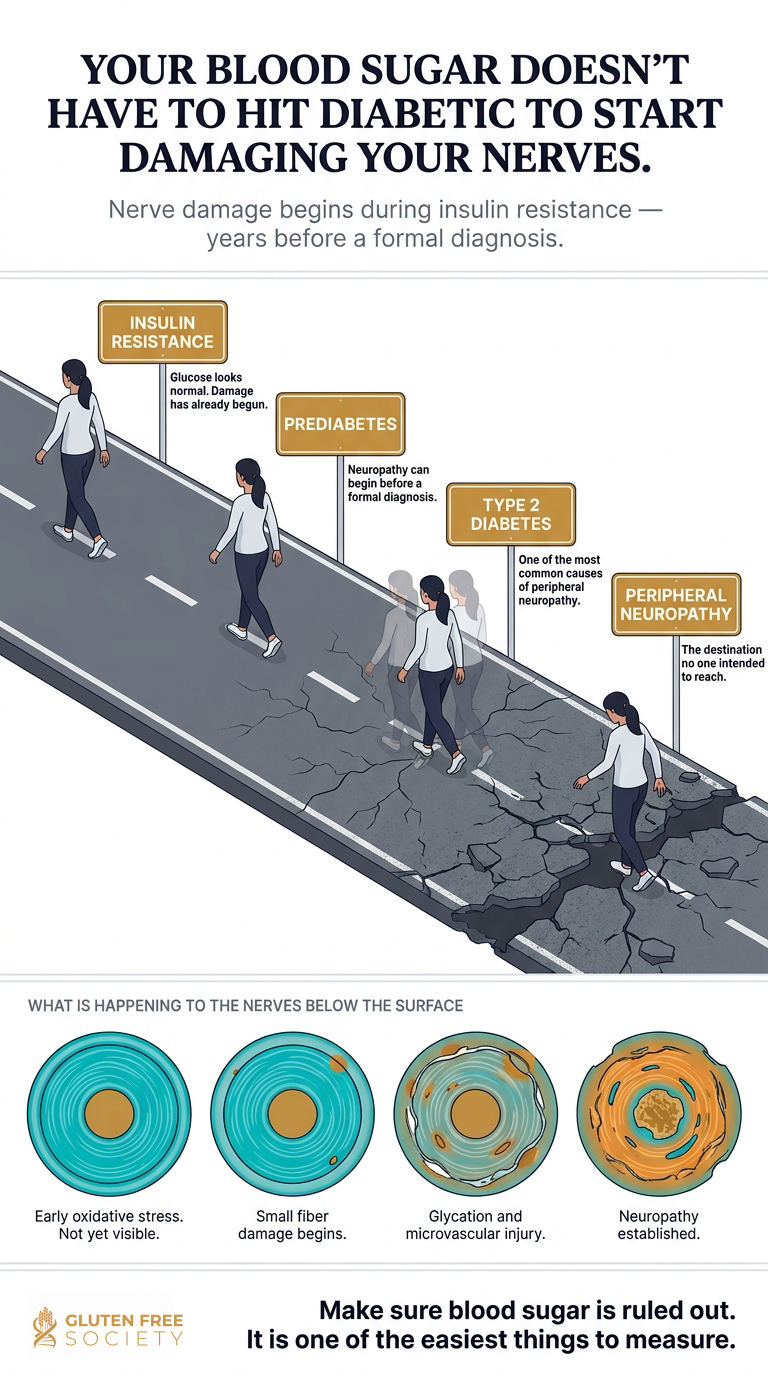
| Blood sugar problems | Glycation, oxidative stress, reduced blood flow, mitochondrial injury | Diabetes, prediabetes, insulin resistance |
| Nutrient deficiency | Poor myelin repair, impaired nerve signaling, low mitochondrial energy | B12, B1, B6, folate, vitamin E, copper, magnesium |
| Gluten-related disease | Malabsorption, immune activation, inflammation, neurological autoimmunity | Celiac disease, non-celiac gluten sensitivity, gluten neuropathy |
| Autoimmune disease | Immune attack on nerves, chronic inflammatory signaling | Sjögren’s, lupus, rheumatoid arthritis, Hashimoto’s, celiac disease |
| Medications | Direct nerve toxicity or nutrient depletion | Metformin, PPIs, chemotherapy, fluoroquinolones, diuretics |
| Alcohol | Direct nerve toxicity and B-vitamin depletion | Chronic alcohol use |
| Toxins | Oxidative stress, mitochondrial injury, nerve poisoning | Heavy metals, solvents, pesticides, chemotherapy |
| Infections | Immune activation or direct nerve injury | Shingles, Lyme disease, HIV, hepatitis C, etc |
| Mechanical compression | Physical pressure on nerves | Carpal tunnel, spinal stenosis, sciatica, tarsal tunnel |
| Digestive disease or surgery | Poor absorption of nerve-supporting nutrients | Celiac disease, IBD, bariatric surgery, gallbladder removal |
| Mold/mycotoxins | Neuroinflammation, immune activation, mitochondrial stress | Water-damaged building exposure |
| Idiopathic | The cause has not been found yet | In my experience, Idiopathic neuropathies are diagnosed when the doctor hasn’t looked into the above triggers thoroughly. |
Type II Diabetes is one of the most common causes of peripheral neuropathy. High blood sugar injures nerves through several mechanisms:
Your nerves are living tissue. They require oxygen, blood flow, mitochondrial energy, antioxidants, healthy fats, amino acids, and micronutrients. When those raw materials are missing, nerve function suffers. There is a robust body of medical literature connecting nutritional deficiency to PN.
Nutritional deficiencies linked to peripheral neuropathy include:
| Nutrient | Why It Matters for Nerves | Deficiency Symptoms That May Overlap With Neuropathy | Best Tests to Consider | Grain-Free Food Sources |
|---|---|---|---|---|
| Vitamin B12 | Myelin, nerve signaling, methylation, red blood cells | Numbness, tingling, weakness, balance issues, anemia, cognitive changes | B12, methylmalonic acid, homocysteine, CBC, Intracellular Nutrient Analysis (INA) | Beef, liver, fish, shellfish, eggs |
| Vitamin B1 / thiamine | Glucose metabolism, nerve energy, mitochondrial function | Burning feet, weakness, fatigue, neuropathy, poor coordination | Whole blood thiamine, transketolase, Intracellular Nutrient Analysis (INA) | Pork, fish, eggs, liver, sunflower seeds |
| Vitamin B6 | Neurotransmitters, amino acid metabolism, nerve function | Numbness, tingling, irritability. Too much can also cause neuropathy | PLP, Intracellular Nutrient Analysis (INA) supplement review | Poultry, fish, beef, organ meats, pistachios |
| Folate | Methylation, red blood cells, nerve repair | Fatigue, anemia, elevated homocysteine, neurological symptoms | Folate, RBC folate, homocysteine, CBC, Intracellular Nutrient Analysis (INA) | Liver, leafy greens, asparagus, avocado |
| Vitamin E | Antioxidant protection, nerve membranes | Ataxia, neuropathy, weakness, poor coordination | Intracellular Nutrient Analysis (INA) | Nuts, seeds, avocado, olive oil |
| Copper | Myelin, iron metabolism, spinal cord and nerve function | Gait problems, neuropathy, anemia, low white blood cells | Copper, ceruloplasmin, Intracellular Nutrient Analysis (INA) | Oysters, liver, shellfish, nuts, seeds |
| Magnesium | Nerve conduction, muscle relaxation, glucose metabolism | Cramps, twitching, weakness, poor blood sugar control | RBC magnesium, Intracellular Nutrient Analysis (INA) | Pumpkin seeds, leafy greens, avocado, cacao |
| Omega-3 fatty acids | Nerve membranes, inflammation balance | Dry skin, inflammation, poor membrane function | Omega-3 index, Intracellular Nutrient Analysis (INA) | Wild salmon, sardines, anchovies, mackerel |
| Vitamin D | Immune regulation, inflammation balance, muscle function | Muscle weakness, immune dysregulation, pain sensitivity | 25-OH vitamin D | Sunlight, fatty fish, eggs |
| Zinc | Immune balance, repair, antioxidant enzymes | Poor healing, immune dysfunction, taste changes | Plasma and RBC zinc, Intracellular Nutrient Analysis (INA) | Oysters, beef, lamb, pumpkin seeds |
| Iron | Oxygen delivery, mitochondrial function | Fatigue, restless legs, weakness, poor exercise tolerance | Ferritin, iron panel, CBC | Red meat, liver, shellfish |
| Protein / amino acids | Tissue repair, neurotransmitters, glutathione, enzymes | Weakness, poor healing, low muscle mass | Total protein, albumin, amino acid testing, Intracellular Nutrient Analysis (INA) | Beef, poultry, fish, eggs, collagen, bone broth |
| Choline | Cell membranes, acetylcholine, methylation | Cognitive issues, liver stress, nerve signaling issues | Intracellular Nutrient Analysis (INA) | Eggs, liver, meat, fish |
| Alpha-lipoic acid | Antioxidant and mitochondrial support | Oxidative stress, metabolic nerve injury | Intracellular Nutrient Analysis (INA) | Spinach, organ meats, red meat in small amounts |
| Acetyl-L-carnitine | Mitochondrial fatty acid transport, nerve energy | Fatigue, poor mitochondrial function, neuropathic pain patterns | Intracellular Nutrient Analysis (INA) | Red meat, lamb, fish |
Gluten-related disease is not confined to the GI tract. Celiac disease and gluten sensitivity can affect the nervous system. Human research has linked celiac disease with peripheral neuropathy, gluten ataxia, and other neurological manifestations. In addition, those without those with non celiac gluten sensitivity (NCGS) can also develop neuropathy. Small-fiber neuropathy has also been described in celiac disease, with some patients reporting improvement on a gluten-free diet. Not only is PN a possible complication of gluten sensitivity, a gluten free diet has been shown to lead to improvements. In my clinical experience, I have seen many patients improve from PN symptoms as they change their diet change and correct nutritional deficiencies.
Possible mechanisms for gluten induced neuropathy include:
Other forms of autoimmune disease can also contribute to neuropathy when the immune system attacks nerve tissue or creates chronic inflammatory injury.
Other Autoimmune drivers of PN may include:
Autoimmune neuropathy may require specialized lab testing and deeper immune evaluation, especially when symptoms are unexplained, painful, asymmetric, rapidly progressive, or accompanied by systemic inflammatory symptoms. If autoimmune inflammation is driving your PN, it is of vital importance that you work with a doctor who can help you identify the four triggers of autoimmune disease:
I discuss these triggers in much greater depth in Chapter 11 of my book, No Grain No Pain. If this is the first time you are hearing about autoimmune triggers, I strongly recommend doing more research on the topic. Beyond neuropathy, autoimmune diseases can take years of life from you if left unchecked.
Some medications can directly injure nerves. Others may increase risk indirectly by depleting nutrients needed for nerve function. Medication-induced nutrient depletion is one of the most overlooked contributors to peripheral neuropathy.
| Medication or Drug Class | Possible Neuropathy Connection | Possible Nutrient Depletion / Mechanism | Practical Consideration |
|---|---|---|---|
| Metformin | May worsen neuropathy risk through B12 depletion | B12, Folate, and CoQ10 depletion, methylation impact | Check B12, folate, and CoQ10 through INA testing. Additional tests to consider: MMA, homocysteine, CBC, nutrient status |
| Proton pump inhibitors | Indirect nerve risk through nutrient depletion | B12, magnesium, iron, calcium, protein digestion | Perform Intracellular Nutrient Analysis (INA) to rule out nutrient insufficiency |
| H2 blockers | Reduced stomach acid may impair nutrient release | B12, minerals, protein digestion | Perform Intracellular Nutrient Analysis (INA) to rule out nutrient insufficiency |
| Statins | Muscle symptoms, mitochondrial concerns in some | CoQ10 pathway effects, muscle symptoms | Perform Intracellular Nutrient Analysis (INA) to rule out nutrient insufficiency |
| Chemotherapy drugs | Direct neurotoxicity | Axonal injury, mitochondrial stress | Neuropathy can be dose-limiting. Perform Intracellular Nutrient Analysis (INA) to rule out nutrient insufficiency |
| Fluoroquinolone antibiotics | Nerve and tendon adverse effects in susceptible people | Mitochondrial stress, oxidative stress | Review exposure history, Perform Intracellular Nutrient Analysis (INA) to rule out nutrient insufficiency |
| Nitrofurantoin | Known neuropathy risk in susceptible patients | Direct toxicity risk, kidney function relevance | Higher caution with long-term use, monitor nutritional status with INA |
| Anticonvulsants | May affect nutrient status | Folate, vitamin D, B vitamins | Monitor nutritional status with INA |
| Steroids | Blood sugar dysregulation, muscle loss | Glucose elevation, protein breakdown, bone/nutrient effects | Track blood sugar and muscle status, monitor nutritional status with INA |
| Diuretics | Can deplete minerals and B1 | Magnesium, potassium, thiamine, zinc | Monitor electrolytes and nutritional status with INA |
| Oral contraceptives | May affect nutrient status | B vitamins, magnesium, zinc | Perform Intracellular Nutrient Analysis (INA) to rule out nutrient insufficiency |
| NSAIDs | Gut irritation and bleeding risk | Iron loss risk, gut effects | Consider gut and iron markers, Perform Intracellular Nutrient Analysis (INA) to rule out nutrient insufficiency |
| Acetaminophen | Glutathione burden | Increased glutathione demand | Consider NAC/glycine/glutathione support where appropriate. Perform Intracellular Nutrient Analysis (INA) to rule out nutrient insufficiency |
| GLP-1 medications | Case Research shows reduced nutritional intake may cause PN related micronutrient issues. | Low intake, nausea, muscle loss risk | Track protein, nutrients, and muscle mass. Perform Intracellular Nutrient Analysis (INA) to rule out nutrient insufficiency |
| Alcohol | Direct neurotoxicity | B1, B12, folate, magnesium depletion | Eliminate when neuropathy is present. Perform Intracellular Nutrient Analysis (INA) to rule out nutrient insufficiency |
Alcohol is a neurological toxin. In addition, chronic alcohol use drives nutritional deficiencies that cause PN. Thiamine, B12, folate, magnesium, and other B vitamins are well studied links to alcohol induced neuropathy. Beyond alcohol, there are numerous toxic exposures that have been shown to drive peripheral neuropathy. Some of the most common include:
If you suspect a toxin driven neuropathy, make sure you discuss your past occupation, hobbies, home exposures, water damage, pesticides, dental or industrial exposures, chemotherapy history, and supplement use.
Infections caused by bacteria, viruses, parasitic, and other microbes can sometimes damage or inflame the peripheral nerves. When this happens, symptoms may show up in different patterns, including a single affected nerve, multiple scattered nerves, widespread numbness or tingling in the hands and feet, nerve root irritation, inflammatory nerve damage, or even motor nerve dysfunction.
Identifying the underlying infection can lead to targeted treatment and significant improvement. That is why infections should be considered when evaluating unexplained peripheral nerve symptoms. Some common infections that contribute to PN include:
Not all neuropathy is systemic. Sometimes nerves are physically compressed due to trauma or repetitive use injuries.
Examples include:
In cases of nerve entrapment, chiropractic care and physical therapy offer non-invasive and effective treatment options. Keep in mind that compression can coexist with nutrient deficiency, diabetes, inflammation, and autoimmune disease.
Some surgical procedures can create the terrain for neuropathy As a matter of fact research estimates that 10-40% of patients experience chronic neuropathic pain after surgery. There is even a name for it – SNPP or surgically induced neuropathic pain. In my experience, and in the experience of others, these cases can occur because the patients having surgery are malnourished prior their procedure. Being malnourished increases the risk of post surgical complications, including PN. Because of this, I have created a nutritional pre/post surgery protocol for those trying to avoid these complications.
The most overlooked category is digestive tract surgeries, especially bariatric procedures, stomach surgery, ileal resection, pancreatic surgery, and gallbladder removal. These can quietly deplete the nutrients nerves require, especially B12, thiamine, copper, vitamin E, magnesium, iron, omega-3 fats, and amino acids.
The clinical mistake is blaming post-surgical numbness, burning, tingling, or weakness on “aging” or calling it idiopathic without investigating nutrient status. After surgery, nerve symptoms should trigger a deeper look at absorption, protein intake, medication use, blood sugar, inflammation, nutrient deficiencies, and post surgical healing complications.
The following diagram illustrates some of the most common surgeries and how they may contribute to PN:
| Surgery / Procedure | How It May Contribute to Neuropathy | Key Nutrients or Mechanisms Involved | Neuropathy Clues to Watch For |
|---|---|---|---|
| Gastric bypass | Reduces stomach size, stomach acid, intrinsic factor exposure, and nutrient absorption | Vitamin B12, B2, thiamine, iron, folate, copper, vitamin D, protein | Numbness, tingling, burning feet, balance problems, weakness, anemia |
| Sleeve gastrectomy | Reduces stomach capacity and can impair protein, B12, iron, and mineral intake | B12, iron, thiamine, folate, protein, magnesium | Fatigue, neuropathy symptoms, poor muscle recovery, weakness |
| Bariatric surgery in general | Rapid weight loss, reduced intake, vomiting, malabsorption, and nutrient depletion can injure nerves | Thiamine, B12, copper, folate, vitamin E, protein | Burning feet, leg weakness, gait problems, confusion, severe fatigue |
| Small intestine resection | Removes absorptive surface area needed for nutrient uptake | B12, folate, magnesium, zinc, iron, amino acids | Tingling, numbness, anemia, diarrhea, weight loss |
| Ileal resection | The ileum is a key absorption site for B12 and bile acids | Vitamin B12, fat-soluble vitamins, bile acid balance | B12 deficiency symptoms, neuropathy, anemia, diarrhea |
| Colon surgery with chronic diarrhea | Can increase fluid, mineral, and electrolyte losses | Magnesium, potassium, zinc, B vitamins, hydration | Cramps, weakness, tingling, fatigue |
| Gallbladder removal | May impair bile flow timing and fat handling in some people | Vitamin E, vitamin D, vitamin K, omega-3 fats, essential fatty acids | Fatty stool, poor fat tolerance, dry skin, nerve symptoms with fat-soluble nutrient deficiency |
| Pancreatic surgery | Can reduce digestive enzyme output and impair fat/protein digestion | Protein, amino acids, vitamin E, vitamin D, omega-3 fats, B vitamins | Weight loss, greasy stool, malnutrition, weakness, neuropathy |
| Stomach surgery / partial gastrectomy | Reduces acid, intrinsic factor, and protein digestion | B12, iron, folate, protein, zinc | Numbness, tingling, anemia, poor healing |
| Fundoplication or anti-reflux surgery | May alter eating patterns, stomach function, or protein digestion in some patients | Protein, B12, iron, minerals | Bloating, early fullness, poor intake, weakness |
| Colectomy with ileostomy | Can increase fluid and mineral losses and alter absorption depending on anatomy | Magnesium, zinc, potassium, sodium, B vitamins | Dehydration, cramps, weakness, tingling |
| Cancer surgery with chemotherapy | Surgery may reduce intake while chemotherapy can directly injure nerves | Direct neurotoxicity, B vitamins, protein, glutathione support | Burning, numbness, tingling after treatment |
| Spinal surgery | Nerve roots may be compressed, irritated, inflamed, or injured before, during, or after surgery | Mechanical nerve injury, scar tissue, inflammation | Radiating pain, weakness, numbness, foot drop |
| Joint replacement or orthopedic surgery | Local nerve compression, traction, swelling, or positioning injury may occur | Mechanical trauma, inflammation, circulation | Numbness near incision, weakness, burning, altered sensation |
| Long surgeries under anesthesia | Prolonged positioning can compress peripheral nerves | Mechanical compression, reduced blood flow | New numbness, tingling, weakness after surgery |
Simply put, idiopathic means that the doctor doesn’t know why the condition is happening. Many people with peripheral neuropathy are misdiagnosed or told their condition is “idiopathic.” But for the patient, that label does not explain what is damaging the nerves.
And once a person is labeled idiopathic, the investigation often stops. Instead of digging deeper into root causes, the conversation shifts toward symptom control with drugs for nerve pain. Those medications may reduce pain signals for some people, but they do not answer the most important question: why are the nerves being damaged in the first place? The real lesson is that polyneuropathy deserves a deeper workup, not a shrug, a label, and a prescription. “Idiopathic” should not be the end of the conversation. It should be the beginning of a better investigation.
PN can be complicated and multifactorial. For this reason alone, many people are given a diagnosis but not an explanation. Determining root cause triggers requires time, attention to detail, a thorough patient history, physical examination, imaging, lab studies, bloodwork, and an experienced and well trained doctor.
In today’s medical economy, doctors are overwhelmed, overworked, overburdened by paperwork, appointments are rushed, insurance creates unnecessary hurdles, and frustrated patients are often left confused and in the dark.
Common reasons include:
Neuropathy is not a gabapentin deficiency, a pregabalin deficiency, or an antidepressant deficiency. Those drugs may reduce symptoms for some people, but they do not answer the root-cause question.
The following is a list of tests and procedures for patients to review before going to their doctor. Sometimes a well informed patient can provide insight that doctors miss. Remember that you and your doctor should be working as a team to determine your diagnosis and path forward.
| Test | What It Measures | Pros | Limitations |
|---|---|---|---|
| Neurological exam | Reflexes, strength, sensation, gait, balance | Foundational exam that provides insight into nerve damage type and location | Does not identify all root causes |
| EMG / nerve conduction study | Large fiber nerve function and muscle response | Useful for large fiber neuropathy, radiculopathy, entrapment | Can miss small fiber neuropathy |
| Skin biopsy | Intraepidermal nerve fiber density | Useful for small fiber neuropathy | Does not identify root cause by itself |
| Quantitative sensory testing | Sensory thresholds | Helpful functional data | Less specific than biopsy |
| Autonomic testing | Sweat, heart rate, blood pressure responses | Useful for autonomic neuropathy | Specialized testing |
| A1c | Average glucose estimate | Useful trend marker | Can miss glucose swings and insulin resistance |
| Fasting glucose | Blood sugar at one point | Easy and inexpensive | Often normal in insulin resistance |
| Fasting insulin | Insulin demand | Detects early metabolic stress | Not always ordered |
| Oral glucose tolerance test | Glucose response over time | Can reveal impaired glucose handling | Requires time and prep |
| B12 | Serum B12 levels | Basic screening | Commonly inaccurate. May miss functional deficiency |
| Methylmalonic acid and Homocysteine | Indirect measurement of B12 status | More specific for B12 need vs. serum testing | Can be affected by kidney function |
| Food Sensitivity Screening | Immune reactions to dietary foods | Identifies possible trigger foods | Many doctors will not order this test |
| Folate | Folate status | Helpful with anemia and methylation | Serum may fluctuate and be inaccurate for true deficiency |
| B1 / thiamine | Thiamine status | Important in diabetes, alcohol, diuretics | Testing varies by method |
| B6 / PLP | Vitamin B6 status | Helps identify deficiency or excess | Must assess supplement intake |
| Vitamin D | 25-OH vitamin D | Immune and musculoskeletal relevance | Not nerve-specific |
| Vitamin E | Fat-soluble antioxidant status | Useful with fat malabsorption | Interpret with lipids |
| Copper and ceruloplasmin | Copper status | Important when gait, anemia, zinc use, surgery history | Often overlooked |
| Magnesium / RBC magnesium | Magnesium status | More useful than serum magnesium alone | RBC not perfect |
| Omega-3 index | EPA/DHA status | Reflects membrane omega-3 status | Not diagnostic for neuropathy |
| Intracellular Nutrient Analysis | Nutrient status inside cells | Helps identify functional nutritional insufficiency to better determine supplement need | Does not identify toxicity |
| Thyroid panel | TSH, T4, T3, antibodies | Screens metabolic and autoimmune thyroid issues | TSH alone may be incomplete |
| Autoimmune markers | ANA, ENA, ESR, CRP, Sjögren’s markers, etc. | Useful with systemic symptoms | Must match clinical picture |
| Celiac/gluten testing | Immune response to gluten and intestinal injury | Important in unexplained neuropathy | Gluten restriction may alter results |
| HLA-DQ genetics | Genetic risk for gluten-related disease | Useful when already gluten-free | Risk marker, not disease diagnosis |
| Heavy metals | Toxic metal exposure | Useful with exposure history | Interpretation requires expertise |
| Mycotoxin testing | Mold-related toxin burden | Useful in context of water-damaged building exposure | Should be performed after following a mold free diet |
In my experience, INA testing is one of the most effective and accurate ways to determine the presence of nutritional insufficiency. Serum laboratory tests that measure vitamins and minerals have a number of pitfalls, and commonly create a false perception of the true nutritional picture.
Great food should be the foundation for healing peripheral neuropathy. As a matter of fact, nutrients provided by food are a non-negotiable for nerve healing and regeneration. Foods and patterns that may interfere with your healing or worsen neuropathy risk include:
Supplements can be valuable tools to support nerve function, nutrient status, mitochondrial health, antioxidant defense, blood sugar metabolism, and inflammatory balance. Because some peripheral neuropathies are caused or worsened by nutritional deficiencies, targeted supplementation may play a role when testing confirms deficiency, insufficiency, malabsorption, medication depletion, or increased demand.
As there are many nutrients involved in nerve health, my recommendation is to test, don’t guess. Nutritional testing can give you a unique and personalized blueprint to follow. The following is a list of some of the most common nutrients linked to nerve health:
| Supplement Category | Why It May Help | Common Forms | Typical Adult Dose Range | Testing / Research Notes |
|---|---|---|---|---|
| Vitamin B12 | Myelin, nerve signaling, methylation | Methylcobalamin, adenosylcobalamin, hydroxocobalamin | 1,000 to 10,000 mcg/day when repleting or supporting neurological needs | Test B12 via INA, methylmalonic acid, and homocysteine. B12 has no established upper limit. Research shows relief for patients with PN. |
| B-complex | Supports multiple nerve pathways | Active B vitamins | 1 serving/day, depending on formula | Assess B vitamin status using INA. Avoid blind high-dose B6, especially pyridoxine HCl. Review total B6 from all supplements. |
| Benfotiamine / thiamine | Glucose metabolism, nerve energy | Benfotiamine, thiamine HCl | 150 to 600 mg/day | Assess with INA. Particularly relevant with blood sugar issues, alcohol use, diuretics, poor diet, or malabsorption. |
| Alpha-lipoic acid | Antioxidant, mitochondrial support | R-lipoic acid, alpha-lipoic acid, thioctic acid | 300 to 600 mg/day; some diabetic neuropathy trials use higher ranges | Assess need with INA. Monitor blood sugar response, especially in patients using glucose-lowering medications. Human diabetic neuropathy studies commonly use 600 mg/day, with some analyses evaluating 600 to 1,800 mg/day. |
| Acetyl-L-carnitine | Mitochondrial energy, nerve support | ALCAR | 500 to 1,000 mg, 2 to 3 times/day | Assess need with INA. Human evidence suggests pain benefit in some neuropathy trials. Trials have used 500 mg three times/day and 1,000 mg three times/day in diabetic neuropathy studies. |
| Omega-3 fatty acids | Membrane health, inflammation balance | EPA/DHA | 1,000 to 3,000 mg/day combined EPA + DHA | Use omega-3 index or INA to assess need. Human research shows benefit for patients with neurological pain. |
| Magnesium | Nerve conduction, muscle relaxation | Glycinate, malate, citrate | 200 to 400 mg/day elemental magnesium | RBC magnesium or intracellular testing. Human research shows that magnesium can reduce neurological pain intensity. |
| Vitamin D | Immune regulation, muscle support | D3 | 2,000 to 10,000 IU/day, adjusted to labs | Test 25-OH vitamin D. Studies link peripheral neuropathy with vitamin D deficiency. |
| Vitamin E | Antioxidant, nerve membrane support | Mixed tocopherols/tocotrienols | 100 to 400 IU/day mixed vitamin E | Assess with INA. Vitamin E deficiency results in damaged nerves. Human studies show nerve protection in patients on chemotherapy. |
| Copper | Myelin and neurological function | Copper glycinate, copper bisglycinate | 1 to 3 mg/day when needed | Assess with ceruloplasmin, serum copper, zinc/copper ratio, or INA. Balance with zinc. Copper deficiency has been linked to PN and myelopathy in humans. |
| Zinc | Immune and repair support | Zinc picolinate, citrate, bisglycinate | 15 to 30 mg/day | Assess with INA. Excess zinc can lower copper. Human research shows zinc repletion can alleviate PN. |
| Vitamin C | Myelin production, antioxidant and detox support | Buffered vitamin C, mineral ascorbates | 500 to 5,000 mg/day, divided | Assess with INA. Higher doses may loosen stool. Case studies show vitamin C deficiency neuropathy resolves with supplementation. |
| CoQ10 | Mitochondrial function, antioxidant support | Ubiquinol, ubiquinone | 100 to 300 mg/day | Assess with INA where available. Statin users are at greater risk for deficiency. CoQ10 promotes nerve regeneration and protection. |
| Amino acids / protein | Repair, glutathione, neurotransmitters | Protein powder, essential amino acids, collagen | Protein: ~1.2 to 1.6 g/kg/day minimum, often higher depending on age, muscle loss, healing demand, and metabolic status. EAAs: 5 to 15 g/day. Collagen: 10 to 20 g/day | Assess total protein intake. Assess individual amino acids with INA. Protein needs may be higher with chronic inflammation drives PN. Human studies link low protein diets to nerve damage. |
For gluten-sensitive patients, the nutrient form matters, but so do the other ingredients in the capsule. Fillers, binders, grain-derived excipients, and hidden contaminants can be a problem for sensitive individuals.
Healing requires lifestyle intervention strategies. The six most important decisions you can make everyday include: Eat a whole food diet, exercise, sleep well, get sunshine daily, filter your air, and filter your water. The following diagram goes a little deeper on these strategies.
| Strategy | Why It Helps Nerves | Practical Starting Point |
|---|---|---|
| Walking | Blood flow, glucose control, mitochondrial function | 10 to 20 minutes after meals if safe |
| Resistance training | Muscle, insulin sensitivity, balance | 2 to 3 days per week |
| Balance work | Fall prevention, proprioception | Supported single-leg stance, PT-guided work |
| Sunlight | Circadian rhythm, vitamin D, mitochondrial signaling | Morning outdoor light |
| Sleep | Repair, blood sugar regulation, pain resilience | Consistent sleep schedule |
| Blood sugar tracking | Identifies triggers and spikes | Glucose meter or CGM where appropriate |
| Eat whole foods | Tissue repair and blood sugar stability | Organic, non packaged, protein with every meal |
| Alcohol Elimination | Reduces direct nerve toxicity and nutrient depletion | Eliminate when neuropathy is active |
| Breathe Clean Air | Reduces inflammatory burden | Address water damage and exposure history |
| Drink Clean Water | Supports hydration, circulation, detoxification, and electrolyte balance | Use filtered water and monitor hydration, especially with sweating, diarrhea, diuretics, or high activity |
**Never underestimate the power of your daily choices and the impact on healing they have. In my clinical experience, patients who take these lifestyle interventions seriously always have better outcomes.
Track:
Ask:
Evaluate:
Consider having an Intracellular Nutrient Analysis to help identify possible nutrient deficiency triggers.
Consider fasting glucose, fasting insulin, A1c, oral glucose tolerance, triglycerides, HDL, C-peptide, and waist circumference.
Consider celiac testing, gluten sensitivity markers, HLA-DQ genetics, autoimmune markers, food sensitivity testing, microbial testing, inflammatory markers, and gut evaluation.
Use food first, add targeted supplementation if needed.
Address gluten, grains, sugar, alcohol, processed foods, food sensitivities, microbial imbalances, toxin exposure, medication-related depletion, and blood sugar instability.
Retesting helps confirm whether the strategy is working.
Track pain, sleep, balance, walking tolerance, numbness, strength, digestion, and blood sugar.
Neuropathy is a warning sign. The label is not the root cause.
Your nerves cannot function without the raw materials required to protect, repair, and maintain their function. They need oxygen, blood flow, mitochondrial energy, healthy fats, amino acids, antioxidants, minerals, and vitamins.
Gluten sensitivity and gut damage can impair absorption and trigger immune-mediated nerve problems. Blood sugar damage can begin before diabetes is officially diagnosed. Medications can deplete nerve-supporting nutrients. Alcohol and toxins can injure nerves directly. Autoimmune disease can attack the nervous system. Mold and environmental exposure can add inflammatory burden in susceptible people.
Before you accept numbness, burning, tingling, or nerve pain as your new normal, ask a better question: Have you identified what is damaging the nerves, and have you measured what your body needs to recover?
Peripheral neuropathy is damage or dysfunction of nerves outside the brain and spinal cord. It can affect sensation, pain, movement, balance, digestion, sweating, heart rate, blood pressure, bladder function, and sexual function.
Early signs often include tingling toes, burning feet, numbness, pins and needles, cold sensations, stabbing pain, or feeling like the feet are asleep. Symptoms often begin in the feet before moving upward.
Neuropathy can feel like burning, tingling, numbness, electric shocks, stabbing pain, crawling sensations, hypersensitivity, coldness, or loss of feeling.
Peripheral neuropathy can be caused by diabetes, prediabetes, nutrient deficiency, celiac disease, gluten sensitivity, autoimmune disease, alcohol, medications, infections, toxins, chemotherapy, thyroid disease, kidney disease, liver disease, and nerve compression.
Yes. Human research links gluten-related disorders, including celiac disease and gluten sensitivity, with peripheral neuropathy, gluten neuropathy, small fiber neuropathy, and ataxia.
Yes. Celiac disease can have neurological manifestations, including peripheral neuropathy. This may occur through malabsorption, nutrient deficiency, immune activation, and inflammation.
Yes. Deficiencies in B12, thiamine, vitamin E, copper, folate, and other nutrients can contribute to neuropathy-like symptoms. B12 and copper deficiency are especially important to evaluate.
Burning feet can be associated with B12 deficiency, thiamine deficiency, B6 problems, diabetes, small fiber neuropathy, alcohol use, toxin exposure, or other causes. Testing is needed to identify the driver.
Yes. Vitamin B12 deficiency can cause neurological changes, including numbness, tingling, balance problems, and nerve dysfunction.
Yes. Excess vitamin B6 from supplements can cause sensory peripheral neuropathy. This is why B6 should not be megadosed blindly.
Small fiber neuropathy affects small pain, temperature, and autonomic nerve fibers. It can cause burning pain, prickling, temperature sensitivity, sweating changes, and autonomic symptoms while standard nerve conduction testing may be normal.
Burning feet at night can occur with small fiber neuropathy, diabetic neuropathy, B vitamin deficiency, gluten-related neuropathy, alcohol-related neuropathy, toxin exposure, or nerve compression.
Yes. Diabetes is common, but neuropathy can also occur from nutrient deficiency, gluten sensitivity, autoimmune disease, medications, infections, toxins, alcohol, chemotherapy, thyroid disease, kidney disease, and compression.
Yes. Nerve symptoms can begin before formal diabetes is diagnosed. Insulin resistance, glucose spikes, oxidative stress, and microvascular injury may develop during the prediabetic stage.
Chemotherapy drugs, some antibiotics, nitrofurantoin, excessive vitamin B6, and other agents can contribute directly. Metformin and acid blockers may contribute indirectly through nutrient depletion, especially B12.
Metformin can contribute to B12 deficiency, and B12 deficiency can contribute to neuropathy. In a person with diabetes, neuropathy may be from blood sugar injury, B12 deficiency, or both.
Yes. According to the American Academy of Neurology, People taking statins were 14 times more likely to develop peripheral neuropathy than people who were not taking statins.
Core testing may include neurological exam, EMG/NCS, skin biopsy for small fiber neuropathy, A1c, fasting glucose, fasting insulin, intracellular nutritional analysis to detect vitamin and mineral deficiencies (INA), thyroid panel, gluten testing, autoimmune markers, and toxin testing when appropriate.
Skin biopsy measuring intraepidermal nerve fiber density is commonly used to confirm small fiber neuropathy. Autonomic testing and quantitative sensory testing may also help.
greens, avocado, pumpkin seeds, bone broth, collagen-rich foods, cruciferous vegetables, low-glycemic berries, olives, and olive oil.
Sugar, refined carbohydrates, alcohol, ultra-processed foods, gluten-containing grains in sensitive people, processed gluten-free foods, industrial seed oils, and low-protein diets may worsen the underlying terrain that contributes to neuropathy.
Common nerve-supportive categories include B12, B-complex, thiamine or benfotiamine, magnesium, omega-3 fats, vitamin D, vitamin E, copper when deficient, alpha-lipoic acid, acetyl-L-carnitine, NAC, amino acids, and curcumin.
Some neuropathy improves when the cause is identified and addressed early, especially when related to deficiency, blood sugar problems, gluten exposure, alcohol, medication depletion, or compression. Long-standing nerve damage may be slower or incomplete.
Nerve healing can take months to years depending on the cause, severity, duration, nutrient status, blood sugar control, inflammation, age, and whether the damaging trigger has been removed.
It can be. Some neuropathies are autoimmune or inflammatory, including neuropathy associated with celiac disease, Sjögren’s, lupus, rheumatoid arthritis, vasculitis, inflammatory bowel disease, and autoimmune small fiber neuropathy.
It can be. Neuropathy can increase fall risk, injury risk, ulcers, burns, infections, weakness, and autonomic complications. Rapidly progressive weakness, stroke-like symptoms, loss of walking ability, or bowel/bladder dysfunction should be evaluated urgently.
Urgent symptoms include sudden one-sided weakness, facial drooping, speech problems, rapid ascending weakness, paralysis, loss of bowel or bladder control, severe back pain with neurological deficits, inability to walk, or rapidly worsening symptoms.




3 Responses
Great read, and confirms what I have been suggesting to my GP, (UK), for years, unfortunately I’ve been getting nowhere until seeing a private nutritionist.
This guide, along with your YouTube videos, is exceedingly helpful!
I’m an 82-year old woman with neuropathy in my feet and debilitating exhaustion. I got shingles in my left eye four years ago this month, and am wondering if that may have caused this. I’m still suffering from post-herpetic neuralgia.
I need to find a physician in the Scottsdale, AZ area to work with me and your guide. Can you provide any referrals? Or can you direct me to a website where I can go to search for one?
Gratefully,
MLee
Hi MLee,
Glad the guide and videos are helping you! If you are open to working remotely, consider reaching out to Dr. Osborne’s clinic, Origins. 281-240-2229