new to the gluten free journey?
Vitamin and mineral deficiencies can mimic or look like many disease states. Common examples include:
This does not mean every disease is “just a deficiency,” but you should be aware of the overlap before you accept a lifelong label that is solvable with diet change or nutritional supplementation. If you haven’t been tested for nutritional deficiencies, talk with a nutritionally trained doctor and find out if a simple vitamin or mineral deficiency is behind your health issue.
Modern medicine is very good at naming disease. It is not always good at identifying the root cause.
A patient walks into a clinic with numbness, burning pain, balance problems, weakness, fatigue, brain fog, depression, bruising, shortness of breath, palpitations, or a strange rash.
The common pathway is predictable:
Sometimes the diagnosis is an accurate representation of the cause (i.e. bacterial infection). However; the vast majority of chronic inflammatory diseases are labeled as idiopathic (unknown cause). Many patients go through medical testing, get a diagnosis, a medical treatment, and a quick dismissal. No mention of nutrition, diet, lifestyle, or environmental triggers despite the fact that these influence heavily why inflammation and disease occur in the first place.
Despite the prevailing rhetoric of conventional medicine, nutritional deficiencies are common. The reason they are missed and overlooked is because doctors are not adequately trained in the nutritional sciences. A problem that has been growing for decades now as nutrition has taken a back seat to pharmacology.
In addition, medical insurance companies base the decision on whether to cover nutritional investigation on the behavior patterns of doctors (often referred to as standard of care). So…if medical schools refuse to teach nutrition, doctors remain ignorant, and it never becomes a meaningful part of medical investigation…
Where does that leave us? Nutritional testing, supplements, counseling, or other related services remain out of pocket expenses.
Common causes of nutritional deficiencies include:
Contrary to popular belief, you can be overweight and malnourished. You can eat plenty of calories and still be deficient. Calories are not vitamins and minerals.
Vitamins, minerals, and nutrients are the “molecular work horses” of the body. They are essential for normal body function, maintenance, healing, and repair. Without them, symptoms ensue, and major illness can follow if a deficiency is not corrected. The following is a list of examples. This list is just the tip of the proverbial iceberg:
When those nutrients are missing, tissues fail. When tissues fail, symptoms appear. When symptoms appear, they often resemble disease.
The core clinical principle is simple:
**Deficiency should be ruled out before a patient is told their symptoms are idiopathic, psychosomatic, untreatable, or permanently progressive.
| Nutrient Deficiency | Can Mimic | Research Example |
|---|---|---|
| Vitamin B12 | Multiple sclerosis, dementia, neuropathy, psychosis, depression, spinal cord disease | Vitamin B12 deficiency presents with MS-like symptoms and other forms of neurological disease. |
| Copper | B12 deficiency, MS-like myelopathy, spinal cord disease, neuropathy | Copper deficiency myelopathy closely mimics subacute combined degeneration from B12 deficiency (Journal of Neurology). |
| Thiamine, B1 | Heart failure, fibromyalgia, CFS, and Guillain Barre Syndrome (GBS) | B1 deficiency presents with neurological damage that looks like GBS. |
| Niacin, B3 | Dementia, depression, psychosis, inflammatory bowel symptoms, skin disease | B3 deficiency can present with psychiatric symptoms and altered mental status. |
| Folate | Psychosis, cognitive decline, anemia, depression-like symptoms | Severe folate deficiency has been reported with reversible psychosis and altered mental status. |
| Vitamin D | Fibromyalgia, inflammatory myopathy, chronic pain, weakness | Severe vitamin D deficiency was reported in a case diagnosed as inflammatory myopathy (Frontiers in Pediatrics). |
| Iron | Chronic fatigue, depression-like symptoms, restless legs, poor exercise tolerance | Iron improved fatigue in non-anemic women with low ferritin (CMAJ). |
| Magnesium | Seizures, arrhythmias, tremor, anxiety-like symptoms, muscle spasms | PPI-induced hypomagnesemia has been linked to cardiac and electrolyte disturbances (Cureus, 2024). |
| Vitamin C | Vasculitis, lupus, arthritis, bleeding disorders | Scurvy has been reported as a lupus mimic (SAGE Open Medical Case Reports). |
| Zinc | Psoriasis, eczema, dermatitis, alopecia, immune dysfunction | Zinc deficiency can cause dermatitis, poor wound healing, alopecia, and immune problems; NIH summarizes zinc’s role in immune function and wound healing (NIH ODS Zinc Fact Sheet). |
| Vitamin E | Friedreich-like ataxia, hereditary ataxia, neuropathy | Ataxia with vitamin E deficiency can resemble Friedreich ataxia (Case Reports in Neurological Medicine). |
| Selenium | Cardiomyopathy, heart failure, muscle disease | Selenium-deficient cardiomyopathy has improved after selenium replacement in case literature (Case Reports in Cardiology). |

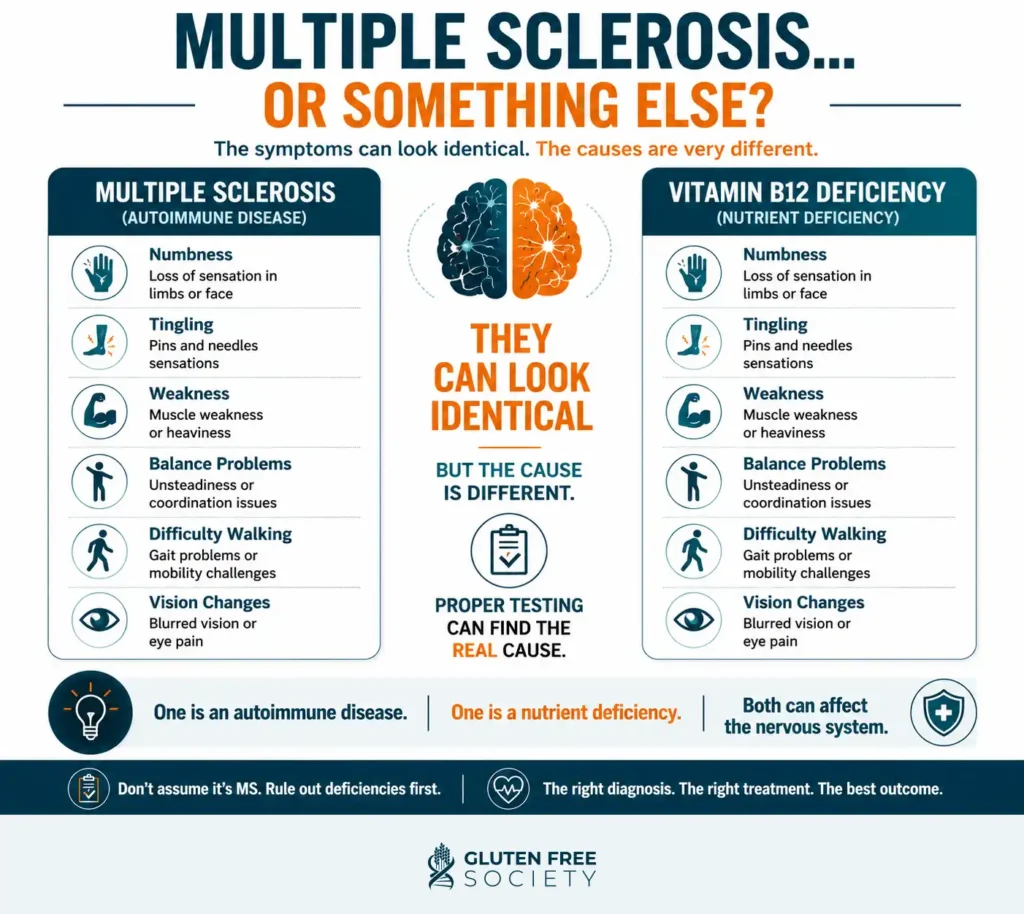
Vitamin B12 deficiency is one of the most important nutrient deficiencies to understand because it can look like a neurological disease, a psychiatric disease, a blood disease, or all three at once.
B12 is required for myelin, the protective insulation around nerves. It is also required for red blood cell formation, DNA synthesis, methylation, and brain chemistry.
When B12 is low, patients can develop numbness, tingling, burning pain, neuropathy, poor balance, weakness, memory loss, brain fog, depression, irritability, hallucinations, psychosis, anemia, glossitis, and fatigue.
In severe cases, B12 deficiency can affect the spinal cord in a condition called subacute combined degeneration. That can produce gait problems, loss of vibration sense, balance problems, and weakness. These symptoms can be mistaken for multiple sclerosis or other spinal cord disorders.
A powerful case example was published in BMJ Case Reports: a patient diagnosed with primary progressive multiple sclerosis was being considered for ocrelizumab, but cervical spine MRI showed findings classic for cobalamin deficiency, including the “inverted V sign.” After parenteral cobalamin treatment, the patient’s neurological symptoms improved quickly and dramatically (BMJ Case Reports, 2019).
A patient with neurological symptoms should not be rushed into a lifelong disease label without a serious evaluation of B12 status. And a common mistake made by doctors is to assess serum B12 only. This test can be misleading and often misses the diagnosis.
Serum B12 tells you how much B12 is floating in the blood. It does not always tell you how well B12 is working inside the cells. Methylmalonic acid, or MMA, and homocysteine can reveal functional problems missed by serum B12. A review in American Family Physician notes that elevated MMA can be used to confirm suspected B12 deficiency when serum B12 is low-normal.
Bottom line: testing only serum B12 is incomplete. A more comprehensive evaluation may include the following lab tests:
A normal CBC does not rule out B12-related neurological injury. Nerve symptoms can occur before anemia appears.
Copper deficiency is another overlooked cause of neurological disease.
Copper deficiency can produce a myelopathy that closely resembles B12 deficiency. A review in the Journal of Neurology described copper deficiency myelopathy as a treatable cause of non-compressive myelopathy that closely mimics subacute combined degeneration from B12 deficiency.
Patients can develop difficulty walking, sensory loss, poor balance, numbness, tingling, weakness, anemia, and low white blood cells.
Copper deficiency is more common in patients with the following medical history:
Another Neurology paper concluded that unrecognized copper deficiency appears to be a cause of idiopathic myelopathy in adults. In patients with myelopathy, neuropathy, gait changes, anemia, or low white blood cells, consider:
Copper deficiency can be treatable, but neurological recovery may be incomplete if it is missed too long. Early detection is critical.
Thiamin, also called vitamin B1, is required to convert food into usable cellular energy. This is especially important for tissues with high energy demand, including the heart, brain, and peripheral nerves. When thiamin is low, the body can lose the ability to efficiently make ATP. When ATP production drops, the heart and nervous system can begin to fail.
This is why thiamin deficiency can mimic two major disease categories:
Classically, thiamin deficiency is called beriberi. There are two major forms. Wet beriberi affects the cardiovascular system and can present with heart failure. Dry beriberi affects the nervous system and can present with neuropathy.
Wet beriberi can look like congestive heart failure because the patient may develop shortness of breath, swelling, rapid heart rate, fluid retention, weakness, low blood pressure, enlarged heart, and signs of poor circulation.
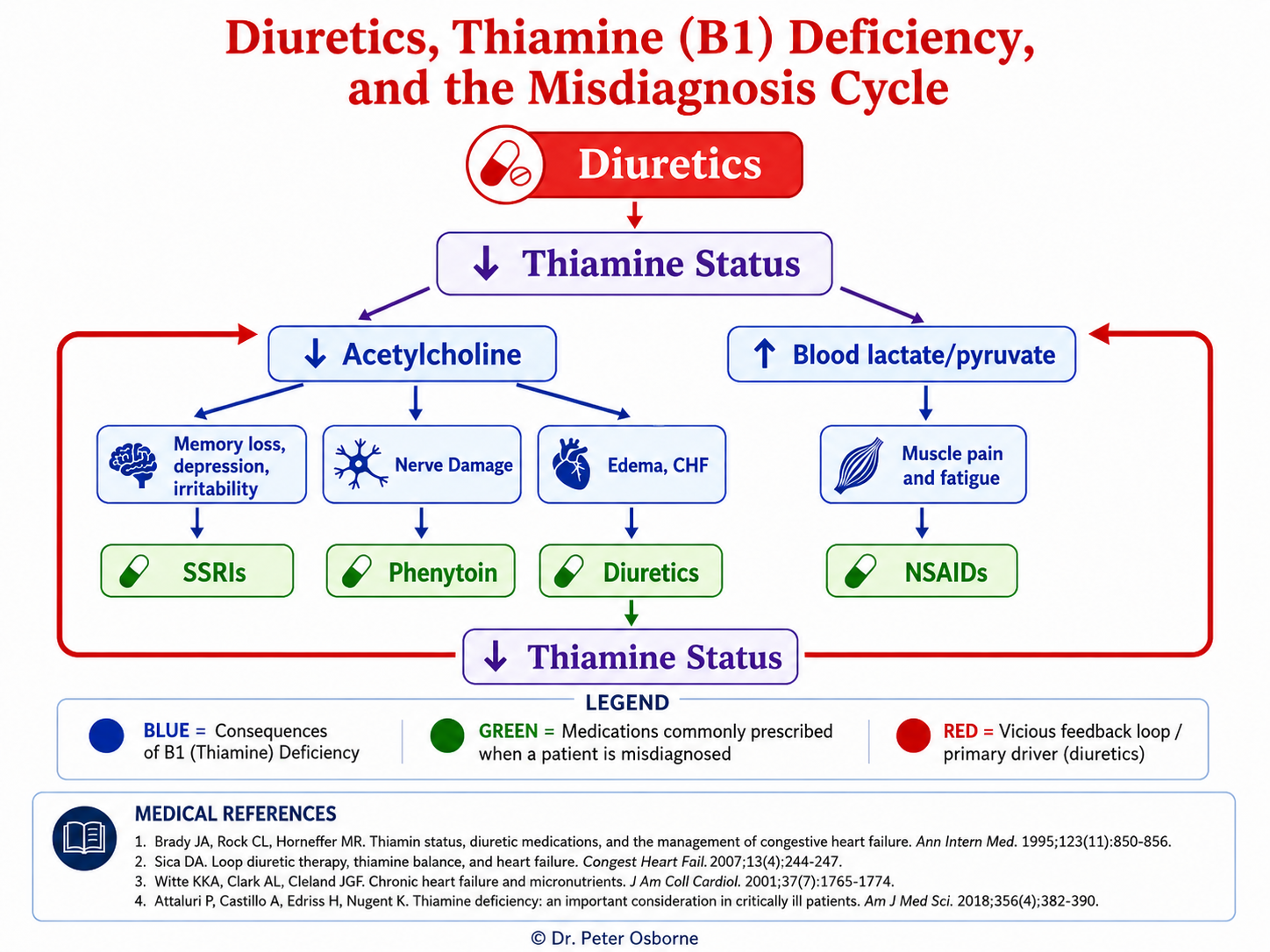
That symptom pattern can easily be labeled as heart failure and treated with medication instead of vitamin B1. This is a major clinical point. One of the medications used to treat heart failure is diuretics.
Diuretics increase fluid loss, but they can also increase urinary loss of water-soluble nutrients, including thiamin. In this scenario, the treatment for the disease increases the circumstance driving the disease.
A meta-analysis on thiamin and cardiac function found that thiamin supplementation may benefit patients with systolic heart failure who are receiving loop diuretics.
For those with heart failure, thiamin status should not be ignored, especially when the patient is on diuretics, has poor nutrition, has a history of alcohol use, has gut disease, has chronic diarrhea, has had bariatric surgery, or has unexplained worsening symptoms.
Dry beriberi affects the peripheral nerves.
This can look like peripheral neuropathy from diabetes, autoimmune disease, spinal disease, medication side effects, or even Guillain-Barré syndrome. Symptoms may include burning pain, numbness, tingling, weakness, difficulty walking, loss of reflexes, and muscle wasting.
A recent case report described thiamin deficiency causing many of the symptoms listed above. Thiamin-related neuropathy is especially important to consider in patients with a history of:
When thiamin deficiency is suspected, testing may include whole blood thiamin, thiamin diphosphate, erythrocyte transketolase activity where available, and blood lactate when severe deficiency is suspected.
In real-world practice, thiamin deficiency rarely presents by itself, it is often found with other B vitamin deficiencies as well. This is one of the reasons I recommend INA testing. It measures vitamin B1 along with the B vitamin complex and related minerals like magnesium.
Thiamin deficiency can look like congestive heart failure. Thiamin deficiency can look like peripheral neuropathy. In some patients, it can look like both at the same time. If you have either diagnosis, ask about vitamin B1.
Niacin, also called vitamin B3, is required to make NAD and NADP, molecules that help drive energy metabolism, DNA repair, and cellular function. Severe niacin deficiency causes pellagra.
The classic triad of symptoms include:
But pellagra does not always present neatly. A patient can show up with psychiatric symptoms, confusion, depression-like symptoms, hallucinations, altered mental status, digestive symptoms, mouth inflammation, and a sun-sensitive rash.
A published case report described a 45-year-old man with pellagra who was initially brought to a psychiatric hospital, illustrating how niacin deficiency can present as mental disorder before the nutritional diagnosis is recognized.
Early onset of vitamin B3 deficiency can present with constipation, bloating, and intestinal pain in the absence of other symptoms.
This is where separate specialists can miss the whole picture. Dermatology sees the rash. Gastroenterology sees loose bowels or diarrhea. Psychiatry sees mood or behavior change. Neurology sees cognitive decline. Each may give a diagnosis and prescribe a medication to treat, never understanding the underlying driver is a simple vitamin deficiency.
Niacin deficiency risk rises with poor diet, alcohol use, malabsorption, chronic diarrhea, inflammatory bowel disease, certain medications, and severe protein deficiency.
Bottom line – Test, don’t guess. Measuring nutritional status could mean the difference between accurate diagnosis and years of unnecessary treatment.
Folate is required for DNA synthesis, methylation, red blood cell production, and nervous system function. Folate deficiency can cause megaloblastic anemia, fatigue, mouth sores, elevated homocysteine, cognitive changes, depression-like symptoms, and psychiatric symptoms.
A published case report described severe folate deficiency presenting with psychosis and altered mental status. The condition completely reversed with folate intervention.
Folate deficiency symptoms can look similar to Crohn’s disease, depression, and pancytopenia (low RBC’s, WBC’s, and platelets).
Folate deficiency can be caused by poor intake, alcohol use, malabsorption, celiac disease, inflammatory bowel disease, pregnancy, methotrexate, anti-seizure medications, certain antibiotics, and high inflammatory burden.
Like other B vitamins, folate should not be evaluated in isolation. It should be interpreted in context with B12. Comprehensive folate status evaluation may include the following:
Vitamin B6 supports neurotransmitter production, hemoglobin formation, immune function, amino acid metabolism, and more than 100 enzyme reactions.
B6 deficiency can look like peripheral neuropathy, seizures, depression-like symptoms, confusion, dermatitis, cracked lips, glossitis, microcytic anemia, and weakened immune function.
If you have been diagnosed with any of these conditions, testing for vitamin B6 deficiency should be performed.
B6 is also a nutrient where excess can injure nerves. High-dose pyridoxine taken long term has been associated with sensory neuropathy, which is why B6 should not be used blindly in high doses.
Vitamin D is commonly discussed as a bone nutrient, but that is only part of the story. Vitamin D also influences muscle function, immune regulation, inflammation, and neurological health.
Severe vitamin D deficiency can present with widespread pain, muscle weakness, bone pain, fatigue, difficulty climbing stairs, poor mobility, and depression-like symptoms.
A case report described a 17-year-old girl with prolonged worsening mobility who was diagnosed with inflammatory myopathy. Her symptoms improved after vitamin D and calcium supplementation.
Additional research has also described how severe vitamin D deficiency can present with musculoskeletal pain and weakness that may be mistaken for other musculoskeletal or mental health conditions.
In my clinical experience, correcting vitamin D deficiency very frequently resolves muscle and joint pain. If you are struggling with muscle weakness, diffuse pain, chronic fatigue, or autoimmune disease have your 25-hydroxy vitamin D levels measured.
Iron is required for oxygen transport, mitochondrial energy production, thyroid function, immune function, brain chemistry, and exercise capacity. Iron deficiency without anemia can contribute to fatigue, poor exercise tolerance, shortness of breath with exertion, hair shedding, restless legs, brain fog, low mood, headaches, dizziness, palpitations, and cold intolerance.
Iron deficiency is one of the most common nutrient deficiencies, and it can exist before anemia shows up on standard lab testing. This is a major medical blind spot. Many patients are told their iron is fine because their hemoglobin is normal. But hemoglobin is late-stage information. Ferritin can drop long before hemoglobin falls.
A randomized controlled trial in CMAJ found that iron supplementation improved fatigue in non-anemic menstruating women with ferritin below 50 mcg/L (CMAJ, 2012). A systematic review in BMJ Open found that iron supplementation in iron-deficient non-anemic adults was associated with reduced subjective fatigue (BMJ Open, 2018).
A case study and literature review described a 42 year old woman who presented to the ER with a 2 month history of fatigue and exertional shortness of breath. Additional testing confirmed that she had cardiomyopathy. Her hemoglobin, MCV, iron, and ferritin levels were low. Treatment with iron resolved her issue. the authors of the study go on to make the following statements:
A complete iron evaluation should include:
In gluten-sensitive patients, iron deficiency is a common problem. Iron is absorbed primarily in the upper small intestine, the same region commonly damaged in celiac disease. Unexplained iron deficiency or treatment non responsive iron deficiency should trigger a deeper look for gluten sensitivity.
Magnesium is involved in hundreds of biochemical reactions. It influences nerves, muscles, blood pressure, glucose metabolism, heart rhythm, mitochondrial energy, and electrolyte balance.
Low magnesium can present with muscle cramps, tremors, twitching, anxiety-like symptoms, insomnia, palpitations, arrhythmias, headaches, seizures in severe cases, low potassium that does not correct, and low calcium that does not correct.
Magnesium deficiency is often missed because serum magnesium can look normal even when total body magnesium is low. Most magnesium is stored inside cells and bone, not floating in the blood.
Long-term proton pump inhibitor use has been associated with hypomagnesemia. A 2024 case report described multiple electrolyte disorders associated with PPI-induced hypomagnesemia, with cardiac manifestations (Cureus, 2024). Another case report described PPI-induced hypomagnesemia causing seizures and cardiomyopathy (J Community Hospital Internal Medicine Perspectives, 2024).
Risk factors include:
Most people think scurvy disappeared with wooden ships and sailors. It did not. Vitamin C deficiency still happens in people with restrictive diets, eating disorders, autism-related food restriction, alcohol use, low fruit and vegetable intake, smoking, inflammatory disease, dialysis, and malabsorption.
Vitamin C is required for collagen production. Collagen supports skin, blood vessels, gums, joints, bones, and connective tissue. When vitamin C is low, blood vessels become fragile and tissues break down.
Deficiency can present with easy bruising, petechiae, bleeding gums, swollen gums, corkscrew hairs, poor wound healing, joint pain, bone pain, fatigue, anemia, and elevated inflammatory markers.
A case report described scurvy initially being mistaken for systemic lupus erythematosus, leading to over-investigation and delayed diagnosis of vitamin C deficiency (SAGE Open Medical Case Reports, 2021).
The clinical clue is the combination of bruising, gum changes, perifollicular bleeding, poor wound healing, joint & muscle pain, and poor diet. This is one of the clearest examples of a deficiency wearing the mask of inflammatory disease.
Zinc is essential for immune function, wound healing, gut barrier integrity, taste and smell, hormone metabolism, DNA synthesis, and skin repair. Zinc deficiency can contribute to dermatitis, psoriasis-like rashes, eczema-like rashes, acne-like lesions, poor wound healing, hair loss, loss of taste or smell, diarrhea, poor immune resilience, low stomach acid, and poor appetite.
Investigating for zinc deficiency should include:
Vitamin E is a fat-soluble antioxidant that helps protect cell membranes and nervous system tissue. Severe vitamin E deficiency can cause ataxia, neuropathy, poor coordination, loss of reflexes, muscle weakness, vision problems, and balance problems.
Ataxia with vitamin E deficiency can resemble Friedreich ataxia. A case report and review described vitamin E deficiency ataxia as a disease with symptoms often resembling Friedreich ataxia, and noted that vitamin E supplementation can improve symptoms (Case Reports in Neurological Medicine, 2022).
Another review emphasized that ataxia with vitamin E deficiency is a diagnosis that should not be missed because it can mimic Friedreich ataxia and is treatable (Annals of Indian Academy of Neurology, 2023).
Vitamin E deficiency is more likely when fat absorption is impaired.
Risk factors include:
If a patient has neuropathy, ataxia, balance problems, and evidence of fat malabsorption, vitamin E should be checked.
Selenium is required for selenoproteins, including glutathione peroxidase and enzymes involved in thyroid hormone conversion. Selenium deficiency can contribute to cardiomyopathy, muscle weakness, thyroid dysfunction, poor antioxidant defense, and immune dysregulation.
A case report described selenium-deficient cardiomyopathy that improved after selenium replacement. Another case report described selenium deficiency causing dilated cardiomyopathy in a child, reinforcing that selenium deficiency can affect cardiac muscle in severe deficiency states.
Large population based studies have shown a connection between increased thyroid disease and low selenium status. Human trials have shown that selenium supplementation can reduce thyroid antibodies in patients with both Grave’s and Hashimoto’s disease.
The takeaway: when cardiomyopathy or autoimmune thyroid disease are medical mysteries, consider having your selenium levels assessed.
Gluten can cause nutritional deficiencies. These nutritional deficiencies can cause symptoms that are often misdiagnosed as non related diseases that lead to medical drug treatments.
Celiac disease is one of the clearest medical examples of how food-triggered immune damage can create nutrient deficiencies. Gluten exposure damages the small intestinal lining in people with celiac disease, impairing absorption of iron, folate, B12, vitamin D, calcium, zinc, magnesium, copper, and other nutrients. A review on micronutrient deficiencies in celiac disease notes that deficiencies can involve iron, folate, B12, vitamin D, zinc, copper, and other nutrients (Nutrients, 2019).
This issue does not stop at celiac disease. Many people with non celiac gluten sensitivity (NCGS) have chronic inflammation, gut symptoms, poor digestion, altered microbial balance, restrictive diets, and nutrient depletion patterns. Even when villous atrophy is not diagnosed, the symptom pattern can still point toward malabsorption or increased nutrient demand.
Nutrient deficiencies in gluten-related disorders can contribute to anemia, neuropathy, fatigue, brain fog, bone loss, muscle pain, depression-like symptoms, hair loss, poor immune function, hormone disruption, and autoimmune flares. This is why a gluten-free diet alone is not always enough.
Removing gluten can stop the inflammatory trigger, but it does not automatically restore depleted nutrients. If a patient has been deficient for years, the tank has to be refilled. The gut has to heal. Absorption has to be reassessed. The diet has to be nutrient-dense, not just gluten-free.
Processed gluten-free foods are often high in starch, sugar, gums, seed oils, and additives. They are frequently low in the nutrients needed for recovery. A gluten-free junk food diet is still a junk food diet.
Another reason deficiencies are missed is that medication side effects are often treated as new diseases. Several commonly used medications can deplete nutrients or interfere with nutrient metabolism.
| Medication Class | Nutrients Commonly Affected | Why It Can Confuse the Picture |
|---|---|---|
| Proton pump inhibitors | Magnesium, B12, iron, calcium | Long-term PPI use has been associated with hypomagnesemia, which can cause cardiac and electrolyte disturbances (Cureus, 2024). |
| Metformin | B12 | Metformin use has been associated with B12 deficiency, which can contribute to neuropathy and cognitive symptoms (Diabetes Care, 2016). |
| Diuretics | Magnesium, potassium, sodium, thiamine, zinc | Diuretics can increase urinary losses of minerals and B vitamins, contributing to cramps, weakness, palpitations, and fatigue. |
| Statins | CoQ10 | Statins inhibit the mevalonate pathway, which is also involved in CoQ10 synthesis; CoQ10 depletion has been proposed as one possible contributor to statin-associated muscle symptoms (Molecules, 2022). |
| Methotrexate | Folate | Methotrexate is a folate antagonist, which is why folate management is commonly part of methotrexate care (StatPearls). |
| Anti-seizure medications | Folate, vitamin D, B vitamins | Some anti-seizure drugs are associated with altered vitamin D and folate status, which can affect bone, mood, and energy. |
| Oral contraceptives | B6, folate, magnesium, zinc in some studies | Oral contraceptive use has been associated with altered micronutrient status in some research, which may contribute to fatigue, mood changes, or headaches in susceptible patients. |
If you are taking any of these medications, it is important to monitor your nutritional status to avoid complications caused by deficiencies.
Nutrient deficiency can mimic disease, but acute symptoms still require proper medical evaluation.
Seek emergency evaluation for:
Root-cause thinking should never delay emergency care. Once the emergency is ruled out or treated, then the deeper investigation can begin.
Finding low nutrients should additionally prompt you to ask more questions. In essence, it is the beginning of the investigation.
Some good questions to start asking yourself:
Food comes first, but food alone is not always enough once a deficiency is clinically significant. A nutrient-dense, gluten-free, whole-food diet should emphasize:
Supplementation should be targeted, tested, and monitored. Don’t try to take everything and hope something helps. Take the right thing, in the right form, in the right amount, for the right reason, and then retest.
You should not have to rely on high doses of supplements for the rest of your life. Recheck your nutritional status periodically. You may find that you need less. You may find that what you need changes over time. Testing provides continued, targeted guidance.
B12, iron, folate, copper, and other deficiencies can produce symptoms before classic anemia appears.
Serum B12 is incomplete. MMA and homocysteine can reveal functional problems missed by serum testing.
Zinc can be helpful, but excess zinc can drive copper deficiency. Balance is the key.
If a patient has iron deficiency, B12 deficiency, vitamin D deficiency, neuropathy, bone loss, or autoimmune disease, gluten-related damage should be considered.
Gluten-free cookies, crackers, cereals, breads, and starches are not recovery foods.
Medication may reduce symptoms, but symptoms are signals. If the body is missing the raw materials for repair, symptom suppression does not rebuild function.
Nutrient deficiencies can mimic disease because the body cannot function without nutrients. A nerve without B12, copper, B6, vitamin E, and essential fats will fail. A muscle without vitamin D, magnesium, potassium, selenium, and protein will fail. A brain without thiamine, B12, folate, iron, magnesium, and healthy fats will fail. A skin barrier without zinc, vitamin C, vitamin A, protein, and essential fats will fail. A heart without magnesium, B1, selenium, thiamine, iron, and mitochondrial support will fail.
When those tissues fail, we name the pattern- (AKA-Disease):
Naming the pattern is not enough when nutritional deficiencies are driving the symptoms. Demand better from your doctor. Get tested. If you doctor won’t test you, find an expert who will.
Yes. Research studies describe nutrient deficiencies mimicking multiple sclerosis, stroke, lupus, vasculitis, psychiatric disease, inflammatory muscle disease, neuropathy, and cardiomyopathy.
Vitamin B12 is one of the most commonly diagnosed neurological mimics. Copper, thiamine, vitamin E, folate, and B6 deficiencies can also drive neurological disease.
Yes. B12 deficiency can damage myelin and spinal cord function, creating symptoms that resemble MS.
Yes. Low ferritin can cause fatigue before hemoglobin drops. In a randomized trial, iron improved fatigue in non-anemic women with low ferritin (CMAJ, 2012).
Severe vitamin D deficiency can cause widespread pain, muscle weakness, fatigue, and poor mobility. Medical literature has shown severe vitamin D deficiency presenting in a way that overlapped with inflammatory muscle disease.
Magnesium deficiency can contribute to tremor, cramps, palpitations, arrhythmias, and nervous system irritability. PPI-induced hypomagnesemia has been reported with cardiac manifestations and electrolyte disturbances (Cureus, 2024).
Yes. Zinc deficiency can contribute to dermatitis, poor wound healing, alopecia, diarrhea, and immune dysfunction.
Gluten-related intestinal damage can impair nutrient absorption. Reviews of celiac disease describe deficiencies involving iron, folate, B12, vitamin D, zinc, copper, and other nutrients.
Not always. You must identify why the deficiency happened. If gluten exposure, medication depletion, chronic diarrhea, low stomach acid, or malabsorption is still present, supplements may not fully correct the issue.
Start with testing. Match the testing to the symptom pattern. Then correct the deficiency, remove the cause, and retest.