new to the gluten free journey?
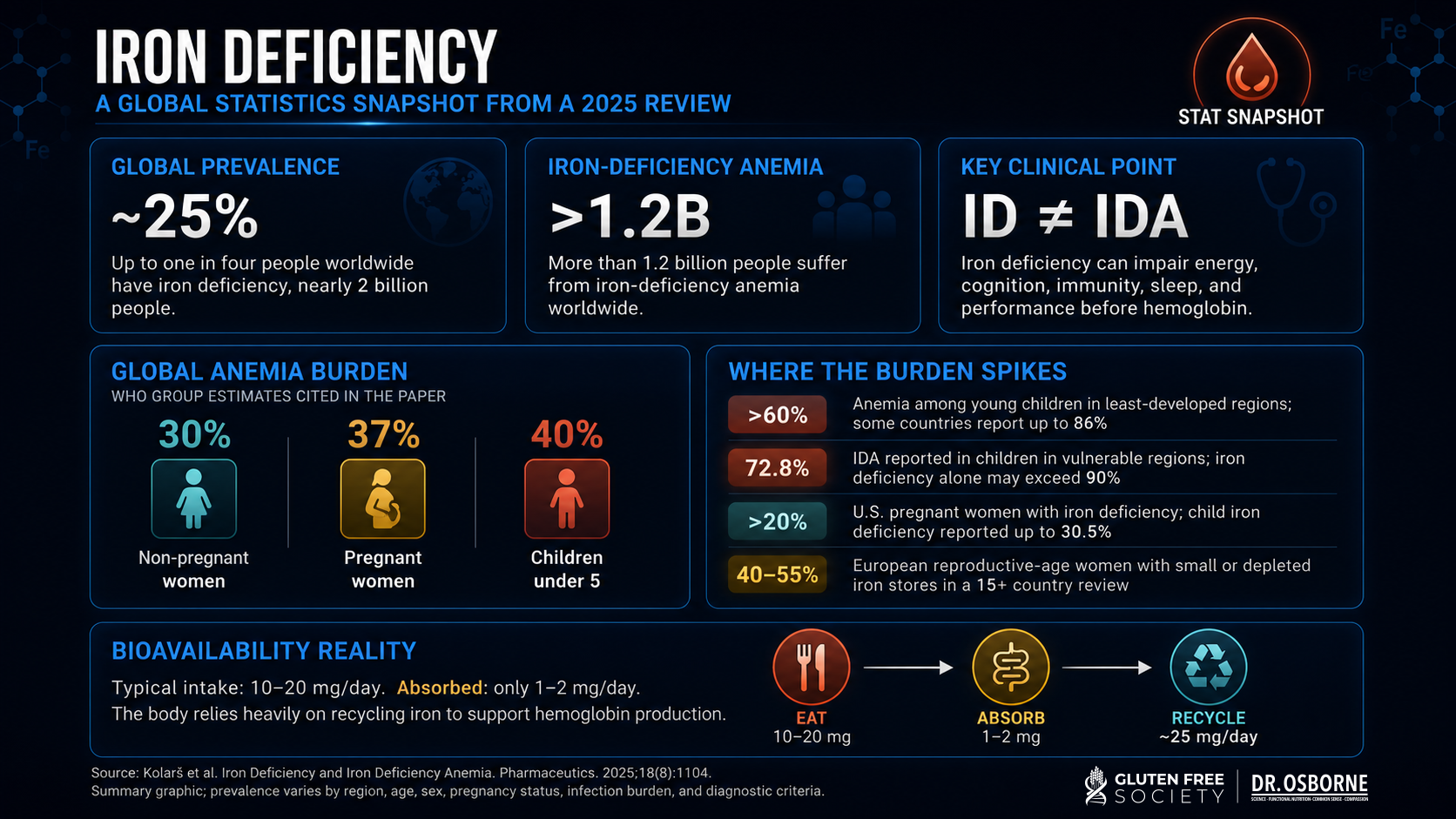
Iron deficiency is the most common nutritional deficiency in the world affecting 25% of the population. More than 1.2 billion have iron deficiency anemia. 30% of women are anemic.
Iron deficiency can be present even in the absence of anemia. This clinical blind spot leads to misdiagnosis for many, because doctors often rely on the use of a CBC test with hemoglobin to diagnose anemia. Iron deficiency without anemia is a common health issue, and fatigue typically shows up before hemoglobin levels falls below the anemia cutoff.
Iron deficiency is more common in those with gluten sensitivity, celiac disease, chronic digestive complaints, heavy menstrual cycles, pregnancy, a history of bariatric surgery, chronic inflammation, or pain medication use.
Iron Deficiency By The Numbers:
| Category | Key Details |
|---|---|
| Nutrient name | Iron |
| Nutrient type | Essential trace mineral |
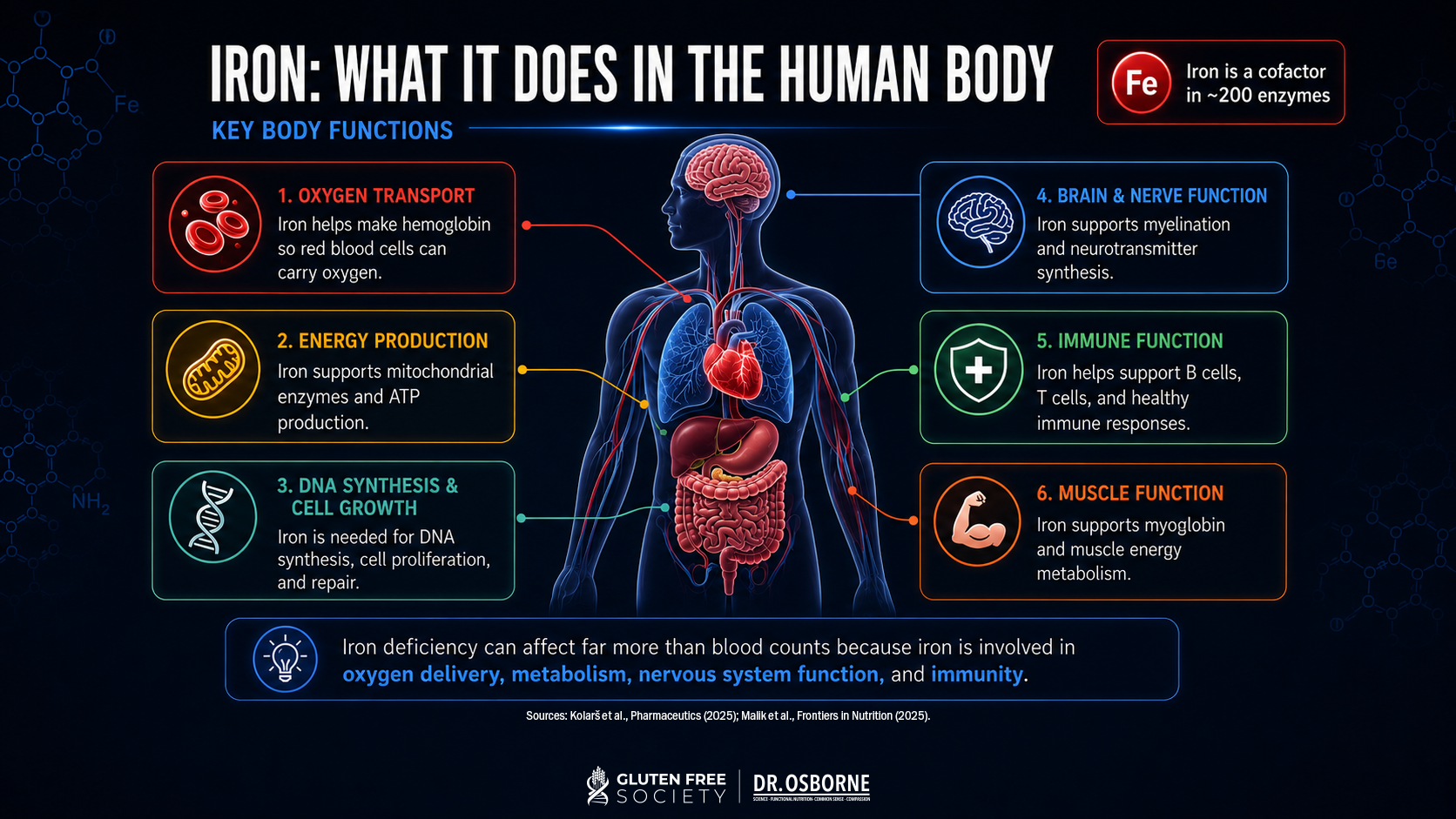
| Main body functions | Oxygen transport, red blood cell production, energy metabolism, mitochondrial function, immune support, thyroid hormone production, brain function |
| Deficiency symptoms | Fatigue, weakness, brain fog, dizziness, shortness of breath, cold intolerance, hair shedding, brittle nails, restless legs, pica, poor exercise tolerance |
| Common depletion causes | Poor intake, blood loss, heavy menstruation, pregnancy, malabsorption, celiac disease, gluten-related gut damage, inflammation, low stomach acid, bariatric surgery, NSAID-related GI bleeding |
| Medications that may contribute | PPIs, H2 blockers, NSAIDs, anticoagulants, aspirin, GLP-1 drugs through reduced intake, some chemotherapy drugs through bleeding or marrow effects |
| Best tests | CBC, ferritin, serum iron, TIBC, transferrin saturation, reticulocyte hemoglobin, CRP/ESR, stool blood testing when indicated |
| Grain-free food sources | Oysters, beef, lamb, bison, liver, sardines, turkey, chicken, eggs, spinach, lentils if tolerated, pumpkin seeds, dark chocolate |
| Supplemental forms | Ferrous aspartate, ferrous sulfate, ferrous gluconate, ferrous fumarate, iron bisglycinate, heme iron polypeptide, carbonyl iron |
| Human research uses | Iron deficiency anemia, iron deficiency without anemia, fatigue, restless legs, pregnancy-related deficiency, bariatric surgery deficiency, pediatric cognition |
| Safe dose range | RDA is 8 mg/day for adult men and women over 50, 18 mg/day for women 19 to 50, and 27 mg/day in pregnancy; adult upper limit is generally 45 mg/day from supplements and food unless medically supervised. |
| Signs of too much | Nausea, constipation, abdominal pain, dark stools, high ferritin, high transferrin saturation, liver stress, iron overload |
| Dr. Osborne Recommended Iron Supplement | Ultra Iron is my supplemental formula designed to support healthy red blood cells with iron plus cofactors including B vitamins, copper, and vitamin C. |
Iron is an essential trace mineral. “Essential” means your body cannot make it, but has to obtain it from food or supplementation. Iron exists in two major dietary forms:
| Form | Found In | Absorption |
|---|---|---|
| Heme iron (Animal Sources) | Meat, poultry, seafood, organ meats | More bioavailable (15-35% can be absorbed) |
| Non-heme iron (Plant based sources) | Vegetables, legumes, nuts, seeds, fortified foods | Less bioavailable and more affected by inhibitors like phytates (~2-20% absorbed) |
Heme iron is more bioavailable than non-heme iron. Vitamin C, meat, poultry, and seafood can improve non-heme iron absorption. Phytates in grains and legumes and some polyphenols can inhibit non-heme iron absorption.
For this reason, a person can “eat iron” and still be deficient. Intake is only one part of the equation. Digestion, stomach acid, gut integrity, inflammation, and absorption determine whether that iron gets into the body and into the cell.
Iron has been used by humans for thousands of years, long before modern chemistry gave it a place on the periodic table. Its importance in human health became clearer as scientists discovered hemoglobin, red blood cells, oxygen transport, and the role of minerals in enzyme systems. The US recognized iron as an essential nutrient in 1941.
Modern nutritional science now recognizes iron as a core biological requirement for oxygen transport, mitochondrial energy production, DNA synthesis, red blood cell production, and immune regulation.
Iron is not just “the anemia nutrient.” Iron affects energy, brain function, thyroid function, immune resilience, muscle performance, pregnancy, growth in children, and nervous system health.
Iron is a central part of the oxygen carrying protein, hemoglobin. Hemoglobin helps red blood cells carry oxygen from the lungs to the tissues. When iron is low, the body cannot deliver oxygen efficiently. That is why iron deficiency can make ordinary life feel exhausting.
Iron is used in mitochondrial enzymes involved in energy production. Low iron can reduce stamina, exercise tolerance, and cellular energy even before anemia appears. Iron deficiency without anemia has been associated with fatigue, and clinical trials show iron supplementation can improve fatigue in some non-anemic women with low ferritin.
Iron is involved in neurotransmitter metabolism, myelin function, and brain development. A 2023 systematic review found that iron deficiency is negatively associated with cognitive development in children and that supplementation can improve their cognitive development.
Iron is part of myoglobin, a protein that helps muscles store and use oxygen. Myoglobin supports oxygen diffusion during muscle activity, which helps explain why low iron can show up as weakness, heavy legs, poor endurance, and reduced exercise capacity.
Iron is needed for thyroid peroxidase, an enzyme involved in thyroid hormone production. A systematic review and meta-analysis found associations between iron deficiency and thyroid dysfunction, although study designs vary and cause-and-effect depends on the patient context.
Iron plays a role in immune system regulation. Too little iron can impair immune function leading to increased risk of infection, while too much free iron can create oxidative stress and support pathogenic growth.
Iron deficiency is multi-factorial. Age, gender, diet, and lifestyle all play a role in the risk for developing iron deficiency.
Common drivers of iron deficiency include:
Beyond the causes listed above, high-risk groups include:
**Celiacs Are at Greater Risk: Iron is absorbed primarily in the duodenum, the first part of the small intestine. That is exactly the area commonly damaged in celiac disease. Research shows that 46% of these patients have iron deficiency and 32% have iron deficiency anemia. For some of these patients, iron deficiency may be the only symptom or abnormal finding.
Medications are one of the most overlooked drivers of iron deficiency. While some medications block iron absorption, others drive GI damage that hinder absorption or cause occult blood loss. If you are taking any of the following commonly prescribed medications, make sure you have your iron levels monitored.
| Medication or Drug Class | How It May Affect Iron | Possible Consequences |
|---|---|---|
| Proton pump inhibitors | Reduce stomach acid, which can impair non-heme iron absorption | Low ferritin, poor response to oral iron, iron deficiency anemia |
| H2 blockers | Suppress gastric acid, potentially reducing iron absorption | Low iron stores over time leading to fatigue and anemia |
| NSAIDs | Can injure the GI lining and cause overt or occult bleeding | Iron deficiency, anemia, fatigue |
| Aspirin | Can injure the GI lining and cause overt or occult bleeding | Low iron, anemia |
| Anticoagulants | Do not deplete iron directly, but can worsen blood loss | Iron deficiency from bleeding |
| GLP-1 medications | May reduce food intake, protein intake, and micronutrient intake (users had 26-30% lower ferritin) | Lower iron intake, lower ferritin risk |
| Chemotherapy drugs | May affect marrow function, appetite, gut lining, or bleeding risk | Anemia, nutrient depletion, poor intake |
| Steroids | Not a classic iron-depleting drug, but can worsen GI risk when combined with NSAIDs | Bleeding risk in some patients |
An estimated 23-45% of patients undergoing a major surgery have pre-existing iron deficiency. The number may climb as high as 80-90% post operatively. After surgery is done, iron is required for healing and repair, and a deficiency can increase the risk for complications.
Beyond the recovery, some surgeries affect the GI tract directly and lead to chronic reduction of iron absorption and deficiency. As surgeries are permanent, you should be informed of the nutritional risks involved. The surgeries listed below are known to contribute to or lead to iron deficiency.
| Surgery | Why It Can Increase Risk |
|---|---|
| Roux-en-Y gastric bypass | Reduces stomach acid and bypasses key absorption areas |
| Sleeve gastrectomy | Reduces stomach capacity and can reduce acid, intake, and tolerance of iron-rich foods |
| Bowel resection | Removes absorptive surface area |
| Duodenal surgery | Directly affects the main iron absorption region |
| Chronic intestinal surgery | Can contribute to malabsorption and inflammation |
| Pancreatic surgery | Can impair digestive enzyme output and nutrient assimilation |
Systematic reviews report that iron deficiency is common after bariatric surgery, with higher risk after malabsorptive procedures such as Roux-en-Y gastric bypass.
Key Takeaway: Medication-induced and surgery-induced nutrient depletion is one of the most overlooked causes of chronic symptoms. Doctors should discuss the risk of iron deficiency, and have a plan to monitor levels periodically.
Because of its many different functions, the symptoms of iron deficiency are varied. The most common symptoms in patients presenting to my functional medicine clinic are fatigue (even with adequate sleep), headaches, muscle pain, exercise intolerance, and restless leg syndrome.
| Body System | Possible Deficiency Symptoms |
|---|---|
| Energy/metabolism | Fatigue, weakness, poor stamina, reduced exercise tolerance |
| Brain/mood | Brain fog, poor focus, dizziness, headaches, anxiety, irritability, depression |
| Nerves | Restless legs, sleep disruption, cold sensitivity |
| Muscles | Muscle pain and weakness, heavy legs, shortness of breath with exertion |
| Skin/hair/nails | Hair shedding, brittle nails, pale skin, spoon-shaped nails, palor |
| Immune system | Poor resilience, frequent infections in some cases |
| Gut/digestion | Sore tongue, cracks at mouth corners, pica, appetite changes |
| Cardiovascular | Palpitations, fast heart rate, heart failure, shortness of breath, and chest discomfort |
| Hormones | Thyroid hormone production may be affected |
| Blood/oxygen transport | Low ferritin, low transferrin saturation, low hemoglobin, microcytic anemia |
The image below represents spooning of the nailbed in a patient with severe muscle pain and fatigue.

A randomized controlled trial in non-anemic women with unexplained fatigue found that 80 mg of elemental iron supplementation daily over 12 weeks improved fatigue in women with ferritin below 50 µg/L.
A BMJ Open systematic review of randomized trials found that iron supplementation improves fatigue in iron-deficient, non-anemic adults.
Key takeaway: fatigue with “normal hemoglobin” should not end the investigation. Ask your doctor to also check ferritin and transferrin saturation.
Iron deficiency anemia is one of the most recognized anemia patterns in celiac disease and may be present in more than half of patients at diagnosis. A meta-analysis found that about 1 in 31 patients with iron deficiency anemia had biopsy-confirmed celiac disease, supporting celiac testing in unexplained iron deficiency anemia.
Clinical takeaway: if iron deficiency keeps coming back, do not just raise the dose. Look for malabsorption and rule out gluten sensitivity as a cause.
Restless legs syndrome is commonly connected to low iron status. Updated consensus recommendations report that oral iron may help patients with restless legs when ferritin is at or below 75 µg/L.
Clinical takeaway: restless legs can be a neurological clue pointing back to iron status.
Iron is connected to thyroid function because the enzyme responsible for building thyroid hormone (thyroid peroxidase) is heme-dependent. Human reviews and meta-analyses have found associations between iron deficiency and thyroid dysfunction.
Clinical takeaway: Thyroid patients with persistent fatigue, hair loss, and cold intolerance should have a full iron panel with ferritin levels checked.
A systematic review in children found that iron deficiency is negatively associated with cognitive development and that supplementation can improve cognitive development in deficient children.
Another review and meta-analysis found that iron supplementation improved intelligence, short term memory, and reduced symptoms of anxiety.
Clinical takeaway: iron affects the brain, not just the blood.
| Goal | Form Used | Dose Range | Duration | Notes |
|---|---|---|---|---|
| General maintenance | Food, multivitamin-level iron | RDA level: 8 mg men and women 51+, 18 mg women 19 to 50 | Ongoing | Needs vary by sex, menstrual status, pregnancy, diet |
| Pregnancy support | Food plus prenatal iron | RDA 27 mg/day | Pregnancy | Monitor at 3-4 month intervals |
| Deficiency correction | Ferrous salts, chelates, heme iron, iron aspartate | Commonly 25 to 65 mg elemental iron/day or alternate-day dosing | 6 to 12+ weeks | Retest ferritin, CBC, TSAT |
| Higher-dose clinical use | Oral or IV iron | Often 60 to 120 mg elemental iron/day orally, or IV under clinical care | Varies | Use when deficiency is documented |
| Restless legs with low ferritin | Often oral iron | 65 mg elemental iron commonly cited | 12 weeks or more | Often considered when ferritin is ≤75 µg/L |
The NIH lists the adult RDA as 8 mg/day for adult men, 18 mg/day for women ages 19 to 50, 8 mg/day for women over 51, and 27 mg/day during pregnancy. Be aware that higher doses of supplemental iron, especially 45 mg/day or more, may cause GI side effects such as nausea and constipation in sensitive people.
Alternate-day dosing can be useful for some people because oral iron supplements can raise hepcidin. This peptide hormone made by the liver can reduce iron absorption. Research has shown that alternate-day dosing may improve fractional iron absorption for some people.
Yes. Iron is essential, but excess iron can be toxic.
| Too Much Iron May Cause | Why It Happens |
|---|---|
| Nausea and constipation | GI irritation from supplemental iron |
| Abdominal pain | Mucosal irritation or excessive dose |
| Dark stools | Common with iron supplementation, but bleeding must be ruled out if symptoms fit |
| High ferritin | Excess storage, inflammation, liver disease, or iron overload |
| High transferrin saturation | Too much circulating iron bound to transferrin |
| Liver stress | Iron overload can deposit in tissues |
| Oxidative stress | Free iron can promote oxidative damage |
Hereditary hemochromatosis and repeated transfusions are major iron overload concerns. Ferritin above 200 µg/L in women or 300 µg/L in men, or transferrin saturation above 40% in women or 50% in men, can justify further evaluation for iron overload.
Key Takeaway: Blind iron supplementation can become problematic. For that reason, testing, correcting deficiency, identifying the cause, and monitoring the response is the smartest choice.
You can use the checklist below to screen yourself for the possibility of iron deficiency, but it is always best to get blood tests to determine the true nature of your situation. A comprehensive list of labs are also listed below, so that you know what you should ask for when visiting your doctor.
| Test | What It Measures | Pros | Limitations |
|---|---|---|---|
| CBC | Hemoglobin, hematocrit, MCV, red blood cell pattern | Detects anemia pattern | Can be normal in early deficiency |
| Ferritin | Stored iron | Best common marker of iron storage | Can rise with inflammation |
| Serum iron | Circulating iron | Part of iron panel | Fluctuates during the day |
| TIBC | Iron-binding capacity | Helps interpret iron demand | Can shift with inflammation |
| Transferrin saturation | Percent of transferrin carrying iron | Useful when ferritin is misleading | Affected by recent intake |
| CRP/ESR | Inflammation | Helps interpret ferritin | Does not measure iron directly |
| Reticulocyte hemoglobin | Iron available for new red blood cells | Can detect early functional deficiency | Not always ordered |
| Soluble transferrin receptor | Cellular iron demand | Less affected by inflammation | Less available |
| Stool occult blood | Hidden GI bleeding | Helps find blood loss | Does not identify all causes |
| Celiac/gluten testing | Malabsorption trigger | Important in refractory low iron | Must be interpreted correctly |
Ferritin below 30 µg/L is commonly used to identify iron deficiency in clinical practice, but ferritin can be falsely elevated in chronic inflammation. In inflammatory states, transferrin saturation below 20% and higher ferritin thresholds may be needed to identify deficiency.
Intracellular Nutrient Analysis (INA) is designed to assess long-term nutrient status inside cells, while conventional serum testing is often a snapshot. For iron, standard blood markers are still essential, but broader nutrient testing can help reveal cofactor deficits that affect red blood cell production and energy.
| Food | Serving Size | Approximate Iron | Notes |
|---|---|---|---|
| Oysters | 3 oz | 8 mg | High-heme iron source |
| Beef liver | 3 oz | 5 mg | Also rich in B12, folate, copper |
| Beef | 3 oz | 2 mg | Heme iron, better absorbed |
| Sardines | 3 oz | 2 mg | Iron plus omega-3s |
| Turkey | 3 oz | 1 mg | Heme iron |
| Chicken | 3 oz | 1 mg | Moderate source |
| Egg | 1 large | 1 mg | Useful but not high-dose |
| Spinach | ½ cup cooked | 3 mg | Non-heme, lower bioavailability |
| Lentils | ½ cup | 3 mg | Non-heme, not ideal for everyone |
| Cashews | 1 oz | 2 mg | Non-heme |
| Dark chocolate | 1 oz | 2 mg | Non-heme, choose low sugar |
Food is foundational. But food may not be enough when:
| Form | Best For | Pros | Cons |
|---|---|---|---|
| Ferrous aspartate | Sensitive stomachs | Amino acid bound form, less side effect prone | Beware of brains with gluten fillers |
| Ferrous gluconate | Lower-dose support | Often gentler | Less elemental iron per tablet |
| Ferrous fumarate | Higher elemental iron | Efficient dosing | Can constipate |
| Iron bisglycinate | Sensitive stomachs | Often well tolerated | Quality varies, beware of fillers |
| Ferrous sulfate | Common clinical use | Well studied, inexpensive | More GI upset, generally less tolerated |
| Heme iron | Absorption support | Less affected by inhibitors | Animal-derived, often costlier |
| Carbonyl iron | Slower release | May be gentler | Slower correction |
| Polysaccharide iron | GI-sensitive patients | Often marketed as gentle | Absorption response varies |
In my clinic, I use ferrous aspartate with patients because I have found it that it does not upset the stomach or cause constipation the way other forms of iron can.
For gluten-sensitive patients, the iron form matters, but so do the other ingredients in the capsule. Fillers, binders, grain-derived excipients, dyes, and hidden contaminants can be a problem for sensitive individuals.
| Cofactor | Why It Matters |
|---|---|
| Vitamin C | Improves non-heme iron absorption |
| Copper | Supports iron transport and utilization |
| Vitamin B12 | Required for healthy red blood cell production |
| Folate | Required for red blood cell formation and DNA synthesis |
| Vitamin B6 | Supports hemoglobin synthesis |
| Protein | Needed to build hemoglobin, transferrin, and tissues |
| Vitamin A | Supports iron mobilization and immune function |
| Magnesium | Supports energy production and red blood cell physiology |
Iron works with other nutrients, and requires copper for transport through the body. Consider using a supplement that also contains copper and B-vitamins for optimal synergy.
Gluten has been shown to contribute to iron deficiency anemia through multiple mechanisms:
Processed gluten-free diets are nutrient-poor. Removing gluten while eating high-starch, low-protein, processed gluten-free substitutes does not rebuild iron stores. For iron recovery, the best diet plan is the No Grain No Pain diet which follows some of the following guidelines:
If you are following a gluten free diet, and looking for a high quality gluten free iron supplement, consider using my formula, Ultra Iron. This is the same supplement I use in my clinic. It is mixed with copper, synergistic B-vitamins, and vitamin C to enhance absorption.
Iron deficiency is the most common nutritional deficiency in the world. Symptoms of deficiency are typically fatigue in the presence of adequate sleep, muscle pain, exercise intolerance, restless legs, brain fog, headaches, dizziness, heart palpitations, shortness of breath, and recurring infections. Testing for iron is easy, but requires a comprehensive evaluation to assess the root cause. Test to identify, change the diet and supplement, look for the cause, re-test.
Iron helps make hemoglobin, carry oxygen, support red blood cell production, maintain energy metabolism, support mitochondrial function, and contribute to brain, immune, muscle, and thyroid function.
Low iron can cause fatigue, weakness, shortness of breath, dizziness, brain fog, cold hands and feet, hair shedding, brittle nails, restless legs, pica, headaches, and poor exercise tolerance.
Yes. Iron deficiency can occur before hemoglobin drops low enough to qualify as anemia. Ferritin and transferrin saturation often reveal the problem earlier than CBC alone.
Ferritin is one of the best common markers of iron stores, but it should be interpreted with CBC, serum iron, TIBC, transferrin saturation, and inflammation markers such as CRP or ESR.
Ferritin below 30 µg/L commonly supports iron deficiency in clinical practice. In chronic inflammation, ferritin can be falsely elevated, and transferrin saturation below 20% becomes especially useful.
Yes. Gluten-related intestinal injury, inflammation, low stomach acid, and malabsorption can contribute to low iron. Celiac disease can present with iron deficiency anemia, sometimes as the only abnormal finding.
Yes. Iron deficiency anemia is common in celiac disease and may occur because the duodenum, the main iron absorption region, becomes damaged.
PPIs and H2 blockers can reduce stomach acid and impair iron absorption. NSAIDs and aspirin can contribute to GI bleeding. Anticoagulants can worsen blood loss. GLP-1 drugs may reduce iron intake through appetite suppression.
Oysters, beef liver, red meat, sardines, turkey, chicken, eggs, spinach, lentils, cashews, pumpkin seeds, and dark chocolate contain iron. Heme iron from animal foods is better absorbed than non-heme iron from plants.
Vitamin C, meat, poultry, and seafood improve non-heme iron absorption. Low stomach acid, phytates, some polyphenols, and calcium can reduce absorption.
The best form depends on tolerance, labs, and response. Ferrous sulfate is well studied, but iron bisglycinate, iron aspartate, heme iron, carbonyl iron, or polysaccharide iron are typically better tolerated.
The RDA is 8 mg/day for adult men and women over 50, 18 mg/day for women ages 19 to 50, and 27 mg/day during pregnancy. Deficiency correction often uses higher targeted doses, guided by testing.
Yes. Too much iron can cause GI side effects and, in susceptible people, iron overload. High ferritin and high transferrin saturation require evaluation before continuing iron.
Iron is often better absorbed on an empty stomach, but many people tolerate it better with food. Avoid taking iron with calcium, coffee, tea, or high-phytate foods when the goal is maximum absorption.
Many people feel changes within weeks, but rebuilding ferritin can take months depending on severity, absorption, ongoing blood loss, inflammation, and dose. Retesting after 6 to 12 weeks is practical.
Iron can help fatigue when deficiency is present. Human trials show iron supplementation can improve fatigue in some non-anemic women with low ferritin.
Iron can help some people with restless legs when ferritin is low. Consensus recommendations often consider iron therapy when ferritin is at or below 75 µg/L.
Iron can be used long term when there is an ongoing need, but labs should be monitored. Long-term blind iron use is not intelligent because excess iron can accumulate in susceptible people.